WO2009132050A9 - Auris formulations for treating otic diseases and conditions - Google Patents
Auris formulations for treating otic diseases and conditions Download PDFInfo
- Publication number
- WO2009132050A9 WO2009132050A9 PCT/US2009/041320 US2009041320W WO2009132050A9 WO 2009132050 A9 WO2009132050 A9 WO 2009132050A9 US 2009041320 W US2009041320 W US 2009041320W WO 2009132050 A9 WO2009132050 A9 WO 2009132050A9
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- agent
- composition
- auris
- agents
- disease
- Prior art date
Links
- 239000000203 mixture Substances 0.000 title claims abstract description 362
- 238000009472 formulation Methods 0.000 title claims abstract description 231
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 title claims description 119
- 201000010099 disease Diseases 0.000 title claims description 60
- 210000005069 ears Anatomy 0.000 title abstract description 50
- 240000006409 Acacia auriculiformis Species 0.000 title abstract description 42
- 238000011282 treatment Methods 0.000 claims abstract description 152
- 238000000034 method Methods 0.000 claims abstract description 48
- 239000002955 immunomodulating agent Substances 0.000 claims abstract description 23
- 239000003795 chemical substances by application Substances 0.000 claims description 143
- 239000003814 drug Substances 0.000 claims description 83
- 208000016354 hearing loss disease Diseases 0.000 claims description 68
- 206010011878 Deafness Diseases 0.000 claims description 65
- 231100000888 hearing loss Toxicity 0.000 claims description 63
- 230000010370 hearing loss Effects 0.000 claims description 63
- 208000012886 Vertigo Diseases 0.000 claims description 60
- 108060008682 Tumor Necrosis Factor Proteins 0.000 claims description 58
- 231100000889 vertigo Toxicity 0.000 claims description 57
- 208000009205 Tinnitus Diseases 0.000 claims description 52
- 231100000886 tinnitus Toxicity 0.000 claims description 51
- 208000027530 Meniere disease Diseases 0.000 claims description 50
- 230000009885 systemic effect Effects 0.000 claims description 37
- 239000005557 antagonist Substances 0.000 claims description 31
- 239000003242 anti bacterial agent Substances 0.000 claims description 31
- 229940127089 cytotoxic agent Drugs 0.000 claims description 29
- 150000003839 salts Chemical class 0.000 claims description 29
- 239000004599 antimicrobial Substances 0.000 claims description 26
- 239000008194 pharmaceutical composition Substances 0.000 claims description 26
- 229940002612 prodrug Drugs 0.000 claims description 26
- 239000000651 prodrug Substances 0.000 claims description 26
- 229940124597 therapeutic agent Drugs 0.000 claims description 25
- 230000001363 autoimmune Effects 0.000 claims description 24
- 239000003112 inhibitor Substances 0.000 claims description 24
- 206010011903 Deafness traumatic Diseases 0.000 claims description 23
- 208000002946 Noise-Induced Hearing Loss Diseases 0.000 claims description 23
- 239000004231 Riboflavin-5-Sodium Phosphate Substances 0.000 claims description 19
- 102100036831 Steroid hormone receptor ERR2 Human genes 0.000 claims description 17
- 239000002158 endotoxin Substances 0.000 claims description 17
- 108091008558 estrogen-related receptor beta Proteins 0.000 claims description 17
- 239000002451 tumor necrosis factor inhibitor Substances 0.000 claims description 17
- 108090000643 Vasopressin Receptors Proteins 0.000 claims description 16
- 102000004136 Vasopressin Receptors Human genes 0.000 claims description 14
- 239000007857 degradation product Substances 0.000 claims description 14
- 229920000428 triblock copolymer Polymers 0.000 claims description 13
- 102000015696 Interleukins Human genes 0.000 claims description 12
- 108010063738 Interleukins Proteins 0.000 claims description 12
- 239000002562 thickening agent Substances 0.000 claims description 12
- 230000001332 colony forming effect Effects 0.000 claims description 11
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Chemical compound O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 claims description 11
- 239000003458 I kappa b kinase inhibitor Substances 0.000 claims description 10
- 230000037396 body weight Effects 0.000 claims description 10
- 208000032625 disorder of ear Diseases 0.000 claims description 10
- 230000002906 microbiologic effect Effects 0.000 claims description 10
- 229940075993 receptor modulator Drugs 0.000 claims description 10
- 239000008223 sterile water Substances 0.000 claims description 10
- 108010035532 Collagen Proteins 0.000 claims description 9
- 102000008186 Collagen Human genes 0.000 claims description 9
- 102000004190 Enzymes Human genes 0.000 claims description 9
- 108090000790 Enzymes Proteins 0.000 claims description 9
- 229920001436 collagen Polymers 0.000 claims description 9
- 239000000463 material Substances 0.000 claims description 9
- 229920002503 polyoxyethylene-polyoxypropylene Polymers 0.000 claims description 9
- 208000023088 sudden sensorineural hearing loss Diseases 0.000 claims description 9
- 102000004868 N-Methyl-D-Aspartate Receptors Human genes 0.000 claims description 8
- 108090001041 N-Methyl-D-Aspartate Receptors Proteins 0.000 claims description 8
- 239000002246 antineoplastic agent Substances 0.000 claims description 8
- 229920001577 copolymer Polymers 0.000 claims description 8
- 108010074605 gamma-Globulins Proteins 0.000 claims description 8
- 238000000520 microinjection Methods 0.000 claims description 8
- 230000000840 anti-viral effect Effects 0.000 claims description 7
- 238000012377 drug delivery Methods 0.000 claims description 7
- 239000012729 immediate-release (IR) formulation Substances 0.000 claims description 7
- 239000000236 nitric oxide synthase inhibitor Substances 0.000 claims description 7
- 231100000057 systemic toxicity Toxicity 0.000 claims description 7
- 102000010637 Aquaporins Human genes 0.000 claims description 6
- 108010063290 Aquaporins Proteins 0.000 claims description 6
- 102000014150 Interferons Human genes 0.000 claims description 6
- 108010050904 Interferons Proteins 0.000 claims description 6
- 239000002111 antiemetic agent Substances 0.000 claims description 6
- 230000003115 biocidal effect Effects 0.000 claims description 6
- 238000011065 in-situ storage Methods 0.000 claims description 6
- 230000003232 mucoadhesive effect Effects 0.000 claims description 6
- 239000003961 penetration enhancing agent Substances 0.000 claims description 6
- 239000012190 activator Substances 0.000 claims description 5
- 229940125683 antiemetic agent Drugs 0.000 claims description 5
- 239000001768 carboxy methyl cellulose Substances 0.000 claims description 5
- 229920002678 cellulose Polymers 0.000 claims description 5
- 239000001913 cellulose Substances 0.000 claims description 5
- 229940122739 Calcineurin inhibitor Drugs 0.000 claims description 4
- 101710192106 Calcineurin-binding protein cabin-1 Proteins 0.000 claims description 4
- 102100024123 Calcineurin-binding protein cabin-1 Human genes 0.000 claims description 4
- 102000010970 Connexin Human genes 0.000 claims description 4
- 108050001175 Connexin Proteins 0.000 claims description 4
- 229940123921 Nitric oxide synthase inhibitor Drugs 0.000 claims description 4
- 229940079172 Osmotic diuretic Drugs 0.000 claims description 4
- 102100040247 Tumor necrosis factor Human genes 0.000 claims description 4
- 229940116211 Vasopressin antagonist Drugs 0.000 claims description 4
- 239000012458 free base Substances 0.000 claims description 4
- 239000003193 general anesthetic agent Substances 0.000 claims description 4
- 229940079322 interferon Drugs 0.000 claims description 4
- 239000002337 osmotic diuretic agent Substances 0.000 claims description 4
- 239000002245 particle Substances 0.000 claims description 4
- 239000002379 progesterone receptor modulator Substances 0.000 claims description 4
- 150000003180 prostaglandins Chemical class 0.000 claims description 4
- 229940076155 protein modulator Drugs 0.000 claims description 4
- 239000003038 vasopressin antagonist Substances 0.000 claims description 4
- 229940123348 ATPase modulator Drugs 0.000 claims description 3
- 229920002134 Carboxymethyl cellulose Polymers 0.000 claims description 3
- 229940125970 Toll-Like Receptor inhibitor Drugs 0.000 claims description 3
- 235000010948 carboxy methyl cellulose Nutrition 0.000 claims description 3
- 239000008112 carboxymethyl-cellulose Substances 0.000 claims description 3
- 230000001362 anti-vertigo Effects 0.000 claims description 2
- KRQUFUKTQHISJB-YYADALCUSA-N 2-[(E)-N-[2-(4-chlorophenoxy)propoxy]-C-propylcarbonimidoyl]-3-hydroxy-5-(thian-3-yl)cyclohex-2-en-1-one Chemical compound CCC\C(=N/OCC(C)OC1=CC=C(Cl)C=C1)C1=C(O)CC(CC1=O)C1CCCSC1 KRQUFUKTQHISJB-YYADALCUSA-N 0.000 claims 1
- 101000795167 Homo sapiens Tumor necrosis factor receptor superfamily member 13B Proteins 0.000 claims 1
- 102100029675 Tumor necrosis factor receptor superfamily member 13B Human genes 0.000 claims 1
- 229940121357 antivirals Drugs 0.000 claims 1
- 210000003027 ear inner Anatomy 0.000 abstract description 158
- 210000000959 ear middle Anatomy 0.000 abstract description 75
- 230000002519 immonomodulatory effect Effects 0.000 abstract description 9
- 230000010412 perfusion Effects 0.000 abstract description 3
- 208000024891 symptom Diseases 0.000 description 63
- 208000035475 disorder Diseases 0.000 description 59
- 230000000694 effects Effects 0.000 description 56
- 102000000852 Tumor Necrosis Factor-alpha Human genes 0.000 description 54
- 208000015181 infectious disease Diseases 0.000 description 53
- 230000006378 damage Effects 0.000 description 48
- 229940079593 drug Drugs 0.000 description 48
- 239000012530 fluid Substances 0.000 description 46
- -1 polymorphs Substances 0.000 description 46
- 239000013543 active substance Substances 0.000 description 44
- 206010033078 Otitis media Diseases 0.000 description 43
- 210000003477 cochlea Anatomy 0.000 description 43
- 210000004027 cell Anatomy 0.000 description 39
- 150000001875 compounds Chemical class 0.000 description 39
- 238000013270 controlled release Methods 0.000 description 38
- 210000003454 tympanic membrane Anatomy 0.000 description 38
- 239000007924 injection Substances 0.000 description 37
- 238000002347 injection Methods 0.000 description 36
- MZOFCQQQCNRIBI-VMXHOPILSA-N (3s)-4-[[(2s)-1-[[(2s)-1-[[(1s)-1-carboxy-2-hydroxyethyl]amino]-4-methyl-1-oxopentan-2-yl]amino]-5-(diaminomethylideneamino)-1-oxopentan-2-yl]amino]-3-[[2-[[(2s)-2,6-diaminohexanoyl]amino]acetyl]amino]-4-oxobutanoic acid Chemical compound OC[C@@H](C(O)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CCCN=C(N)N)NC(=O)[C@H](CC(O)=O)NC(=O)CNC(=O)[C@@H](N)CCCCN MZOFCQQQCNRIBI-VMXHOPILSA-N 0.000 description 33
- 230000001720 vestibular Effects 0.000 description 33
- 210000004379 membrane Anatomy 0.000 description 32
- 239000012528 membrane Substances 0.000 description 32
- 230000004054 inflammatory process Effects 0.000 description 29
- 206010061218 Inflammation Diseases 0.000 description 28
- 210000002768 hair cell Anatomy 0.000 description 28
- 229940125703 otic agent Drugs 0.000 description 27
- 230000033001 locomotion Effects 0.000 description 26
- 230000006870 function Effects 0.000 description 25
- 206010033072 otitis externa Diseases 0.000 description 25
- 230000002411 adverse Effects 0.000 description 24
- 208000027625 autoimmune inner ear disease Diseases 0.000 description 24
- 210000003060 endolymph Anatomy 0.000 description 24
- CMSMOCZEIVJLDB-UHFFFAOYSA-N Cyclophosphamide Chemical compound ClCCN(CCCl)P1(=O)NCCCO1 CMSMOCZEIVJLDB-UHFFFAOYSA-N 0.000 description 22
- 239000000975 dye Substances 0.000 description 22
- 210000004049 perilymph Anatomy 0.000 description 22
- 230000013707 sensory perception of sound Effects 0.000 description 22
- 239000002254 cytotoxic agent Substances 0.000 description 21
- 231100000599 cytotoxic agent Toxicity 0.000 description 21
- 230000002970 ototoxic effect Effects 0.000 description 21
- 206010011891 Deafness neurosensory Diseases 0.000 description 20
- 235000002639 sodium chloride Nutrition 0.000 description 20
- 208000009966 Sensorineural Hearing Loss Diseases 0.000 description 19
- 238000010171 animal model Methods 0.000 description 19
- 210000002569 neuron Anatomy 0.000 description 19
- 239000003642 reactive oxygen metabolite Substances 0.000 description 19
- 231100000879 sensorineural hearing loss Toxicity 0.000 description 19
- FBOZXECLQNJBKD-ZDUSSCGKSA-N L-methotrexate Chemical compound C=1N=C2N=C(N)N=C(N)C2=NC=1CN(C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 FBOZXECLQNJBKD-ZDUSSCGKSA-N 0.000 description 18
- 206010028980 Neoplasm Diseases 0.000 description 18
- 210000000883 ear external Anatomy 0.000 description 18
- 208000023573 sensorineural hearing loss disease Diseases 0.000 description 18
- 208000023275 Autoimmune disease Diseases 0.000 description 17
- 210000003128 head Anatomy 0.000 description 17
- 238000007910 systemic administration Methods 0.000 description 17
- 201000000200 vestibular neuronitis Diseases 0.000 description 17
- 206010008642 Cholesteatoma Diseases 0.000 description 16
- PMATZTZNYRCHOR-CGLBZJNRSA-N Cyclosporin A Chemical compound CC[C@@H]1NC(=O)[C@H]([C@H](O)[C@H](C)C\C=C\C)N(C)C(=O)[C@H](C(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@@H](C)NC(=O)[C@H](C)NC(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](C(C)C)NC(=O)[C@H](CC(C)C)N(C)C(=O)CN(C)C1=O PMATZTZNYRCHOR-CGLBZJNRSA-N 0.000 description 16
- 208000014674 injury Diseases 0.000 description 16
- 231100000199 ototoxic Toxicity 0.000 description 16
- 229940088710 antibiotic agent Drugs 0.000 description 15
- 229960004397 cyclophosphamide Drugs 0.000 description 15
- 239000000499 gel Substances 0.000 description 15
- 208000000509 infertility Diseases 0.000 description 15
- 230000036512 infertility Effects 0.000 description 15
- 208000021267 infertility disease Diseases 0.000 description 15
- 229960000485 methotrexate Drugs 0.000 description 15
- 239000008177 pharmaceutical agent Substances 0.000 description 15
- 210000001050 stape Anatomy 0.000 description 15
- UEJJHQNACJXSKW-UHFFFAOYSA-N 2-(2,6-dioxopiperidin-3-yl)-1H-isoindole-1,3(2H)-dione Chemical compound O=C1C2=CC=CC=C2C(=O)N1C1CCC(=O)NC1=O UEJJHQNACJXSKW-UHFFFAOYSA-N 0.000 description 14
- 241000894006 Bacteria Species 0.000 description 14
- 208000027601 Inner ear disease Diseases 0.000 description 14
- 102000000589 Interleukin-1 Human genes 0.000 description 14
- 108010002352 Interleukin-1 Proteins 0.000 description 14
- 208000017119 Labyrinth disease Diseases 0.000 description 14
- 239000003963 antioxidant agent Substances 0.000 description 14
- 235000006708 antioxidants Nutrition 0.000 description 14
- 210000003169 central nervous system Anatomy 0.000 description 14
- 238000011161 development Methods 0.000 description 14
- 230000018109 developmental process Effects 0.000 description 14
- 210000000613 ear canal Anatomy 0.000 description 14
- 210000005036 nerve Anatomy 0.000 description 14
- 210000003582 temporal bone Anatomy 0.000 description 14
- 210000001213 vestibule labyrinth Anatomy 0.000 description 14
- 108010036949 Cyclosporine Proteins 0.000 description 13
- 208000009129 Ear Neoplasms Diseases 0.000 description 13
- 108010008165 Etanercept Proteins 0.000 description 13
- 206010042674 Swelling Diseases 0.000 description 13
- QJJXYPPXXYFBGM-LFZNUXCKSA-N Tacrolimus Chemical compound C1C[C@@H](O)[C@H](OC)C[C@@H]1\C=C(/C)[C@@H]1[C@H](C)[C@@H](O)CC(=O)[C@H](CC=C)/C=C(C)/C[C@H](C)C[C@H](OC)[C@H]([C@H](C[C@H]2C)OC)O[C@@]2(O)C(=O)C(=O)N2CCCC[C@H]2C(=O)O1 QJJXYPPXXYFBGM-LFZNUXCKSA-N 0.000 description 13
- 239000000427 antigen Substances 0.000 description 13
- 108091007433 antigens Proteins 0.000 description 13
- 102000036639 antigens Human genes 0.000 description 13
- 230000001684 chronic effect Effects 0.000 description 13
- 208000002173 dizziness Diseases 0.000 description 13
- 230000028993 immune response Effects 0.000 description 13
- 238000004519 manufacturing process Methods 0.000 description 13
- 230000008961 swelling Effects 0.000 description 13
- 229960003433 thalidomide Drugs 0.000 description 13
- 208000036142 Viral infection Diseases 0.000 description 12
- 230000000845 anti-microbial effect Effects 0.000 description 12
- 230000004064 dysfunction Effects 0.000 description 12
- 230000001965 increasing effect Effects 0.000 description 12
- 102000005962 receptors Human genes 0.000 description 12
- 108020003175 receptors Proteins 0.000 description 12
- 210000002480 semicircular canal Anatomy 0.000 description 12
- 239000011734 sodium Substances 0.000 description 12
- 150000003431 steroids Chemical class 0.000 description 12
- 241000197194 Bulla Species 0.000 description 11
- 102000004127 Cytokines Human genes 0.000 description 11
- 108090000695 Cytokines Proteins 0.000 description 11
- 102000004310 Ion Channels Human genes 0.000 description 11
- 108090000862 Ion Channels Proteins 0.000 description 11
- 206010023567 Labyrinthitis Diseases 0.000 description 11
- 208000002193 Pain Diseases 0.000 description 11
- GXBMIBRIOWHPDT-UHFFFAOYSA-N Vasopressin Natural products N1C(=O)C(CC=2C=C(O)C=CC=2)NC(=O)C(N)CSSCC(C(=O)N2C(CCC2)C(=O)NC(CCCN=C(N)N)C(=O)NCC(N)=O)NC(=O)C(CC(N)=O)NC(=O)C(CCC(N)=O)NC(=O)C1CC1=CC=CC=C1 GXBMIBRIOWHPDT-UHFFFAOYSA-N 0.000 description 11
- 102000002852 Vasopressins Human genes 0.000 description 11
- 206010047700 Vomiting Diseases 0.000 description 11
- KBZOIRJILGZLEJ-LGYYRGKSSA-N argipressin Chemical compound C([C@H]1C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CSSC[C@@H](C(N[C@@H](CC=2C=CC(O)=CC=2)C(=O)N1)=O)N)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCN=C(N)N)C(=O)NCC(N)=O)C1=CC=CC=C1 KBZOIRJILGZLEJ-LGYYRGKSSA-N 0.000 description 11
- 230000004888 barrier function Effects 0.000 description 11
- 230000027455 binding Effects 0.000 description 11
- 208000002352 blister Diseases 0.000 description 11
- 210000000988 bone and bone Anatomy 0.000 description 11
- 230000007423 decrease Effects 0.000 description 11
- 230000007547 defect Effects 0.000 description 11
- 229960000403 etanercept Drugs 0.000 description 11
- 208000027866 inflammatory disease Diseases 0.000 description 11
- 230000036407 pain Effects 0.000 description 11
- 229960003726 vasopressin Drugs 0.000 description 11
- 208000012639 Balance disease Diseases 0.000 description 10
- 241000700199 Cavia porcellus Species 0.000 description 10
- 230000008901 benefit Effects 0.000 description 10
- 208000005457 endolymphatic hydrops Diseases 0.000 description 10
- 229960000598 infliximab Drugs 0.000 description 10
- 239000002207 metabolite Substances 0.000 description 10
- 239000002510 pyrogen Substances 0.000 description 10
- 230000004044 response Effects 0.000 description 10
- 230000001953 sensory effect Effects 0.000 description 10
- 229960001967 tacrolimus Drugs 0.000 description 10
- QJJXYPPXXYFBGM-SHYZHZOCSA-N tacrolimus Natural products CO[C@H]1C[C@H](CC[C@@H]1O)C=C(C)[C@H]2OC(=O)[C@H]3CCCCN3C(=O)C(=O)[C@@]4(O)O[C@@H]([C@H](C[C@H]4C)OC)[C@@H](C[C@H](C)CC(=C[C@@H](CC=C)C(=O)C[C@H](O)[C@H]2C)C)OC QJJXYPPXXYFBGM-SHYZHZOCSA-N 0.000 description 10
- 208000035143 Bacterial infection Diseases 0.000 description 9
- 102000001284 I-kappa-B kinase Human genes 0.000 description 9
- 108060006678 I-kappa-B kinase Proteins 0.000 description 9
- 108010002350 Interleukin-2 Proteins 0.000 description 9
- 102000000588 Interleukin-2 Human genes 0.000 description 9
- WHUUTDBJXJRKMK-VKHMYHEASA-N L-glutamic acid Chemical compound OC(=O)[C@@H](N)CCC(O)=O WHUUTDBJXJRKMK-VKHMYHEASA-N 0.000 description 9
- 206010036626 Presbyacusis Diseases 0.000 description 9
- 108010004977 Vasopressins Proteins 0.000 description 9
- 241000700605 Viruses Species 0.000 description 9
- 208000027418 Wounds and injury Diseases 0.000 description 9
- 238000009825 accumulation Methods 0.000 description 9
- 229960002964 adalimumab Drugs 0.000 description 9
- 230000000844 anti-bacterial effect Effects 0.000 description 9
- 239000003443 antiviral agent Substances 0.000 description 9
- 208000022362 bacterial infectious disease Diseases 0.000 description 9
- 210000000721 basilar membrane Anatomy 0.000 description 9
- 239000003246 corticosteroid Substances 0.000 description 9
- 229930195712 glutamate Natural products 0.000 description 9
- 239000000546 pharmaceutical excipient Substances 0.000 description 9
- 235000013855 polyvinylpyrrolidone Nutrition 0.000 description 9
- 229920000036 polyvinylpyrrolidone Polymers 0.000 description 9
- 230000009467 reduction Effects 0.000 description 9
- 150000003384 small molecules Chemical class 0.000 description 9
- 239000000126 substance Substances 0.000 description 9
- 230000001988 toxicity Effects 0.000 description 9
- 231100000419 toxicity Toxicity 0.000 description 9
- 230000008673 vomiting Effects 0.000 description 9
- OCJYIGYOJCODJL-UHFFFAOYSA-N Meclizine Chemical compound CC1=CC=CC(CN2CCN(CC2)C(C=2C=CC=CC=2)C=2C=CC(Cl)=CC=2)=C1 OCJYIGYOJCODJL-UHFFFAOYSA-N 0.000 description 8
- 206010028813 Nausea Diseases 0.000 description 8
- 206010033109 Ototoxicity Diseases 0.000 description 8
- 229940126575 aminoglycoside Drugs 0.000 description 8
- 229960001265 ciclosporin Drugs 0.000 description 8
- DQLATGHUWYMOKM-UHFFFAOYSA-L cisplatin Chemical compound N[Pt](N)(Cl)Cl DQLATGHUWYMOKM-UHFFFAOYSA-L 0.000 description 8
- 229960004316 cisplatin Drugs 0.000 description 8
- 210000000860 cochlear nerve Anatomy 0.000 description 8
- 229960001334 corticosteroids Drugs 0.000 description 8
- 229930182912 cyclosporin Natural products 0.000 description 8
- 231100000433 cytotoxic Toxicity 0.000 description 8
- 230000001472 cytotoxic effect Effects 0.000 description 8
- 229940047652 ear drops Drugs 0.000 description 8
- 210000002388 eustachian tube Anatomy 0.000 description 8
- 230000000813 microbial effect Effects 0.000 description 8
- 230000008693 nausea Effects 0.000 description 8
- 206010029864 nystagmus Diseases 0.000 description 8
- 210000000056 organ Anatomy 0.000 description 8
- 208000005923 otitis media with effusion Diseases 0.000 description 8
- 231100000262 ototoxicity Toxicity 0.000 description 8
- 239000001267 polyvinylpyrrolidone Substances 0.000 description 8
- 108090000623 proteins and genes Proteins 0.000 description 8
- UCSJYZPVAKXKNQ-HZYVHMACSA-N streptomycin Chemical compound CN[C@H]1[C@H](O)[C@@H](O)[C@H](CO)O[C@H]1O[C@@H]1[C@](C=O)(O)[C@H](C)O[C@H]1O[C@@H]1[C@@H](NC(N)=N)[C@H](O)[C@@H](NC(N)=N)[C@H](O)[C@H]1O UCSJYZPVAKXKNQ-HZYVHMACSA-N 0.000 description 8
- 238000012360 testing method Methods 0.000 description 8
- 238000002560 therapeutic procedure Methods 0.000 description 8
- 230000009385 viral infection Effects 0.000 description 8
- 230000003612 virological effect Effects 0.000 description 8
- 241000282412 Homo Species 0.000 description 7
- 241001465754 Metazoa Species 0.000 description 7
- 229930182555 Penicillin Natural products 0.000 description 7
- 208000028911 Temporomandibular Joint disease Diseases 0.000 description 7
- 108060008683 Tumor Necrosis Factor Receptor Proteins 0.000 description 7
- 230000004913 activation Effects 0.000 description 7
- 229940121375 antifungal agent Drugs 0.000 description 7
- 229940049706 benzodiazepine Drugs 0.000 description 7
- 210000004556 brain Anatomy 0.000 description 7
- 239000000969 carrier Substances 0.000 description 7
- 239000003085 diluting agent Substances 0.000 description 7
- 229940088598 enzyme Drugs 0.000 description 7
- 210000004209 hair Anatomy 0.000 description 7
- 230000013632 homeostatic process Effects 0.000 description 7
- 238000001802 infusion Methods 0.000 description 7
- 150000002500 ions Chemical class 0.000 description 7
- 210000000265 leukocyte Anatomy 0.000 description 7
- 150000002960 penicillins Chemical class 0.000 description 7
- 208000009800 presbycusis Diseases 0.000 description 7
- 150000003254 radicals Chemical class 0.000 description 7
- 230000002441 reversible effect Effects 0.000 description 7
- 206010039073 rheumatoid arthritis Diseases 0.000 description 7
- 238000001356 surgical procedure Methods 0.000 description 7
- 208000011580 syndromic disease Diseases 0.000 description 7
- 230000001225 therapeutic effect Effects 0.000 description 7
- 230000008733 trauma Effects 0.000 description 7
- 102000003298 tumor necrosis factor receptor Human genes 0.000 description 7
- 210000000752 vestibulocochlear nerve Anatomy 0.000 description 7
- HVAUUPRFYPCOCA-AREMUKBSSA-N 2-O-acetyl-1-O-hexadecyl-sn-glycero-3-phosphocholine Chemical compound CCCCCCCCCCCCCCCCOC[C@@H](OC(C)=O)COP([O-])(=O)OCC[N+](C)(C)C HVAUUPRFYPCOCA-AREMUKBSSA-N 0.000 description 6
- 241000700198 Cavia Species 0.000 description 6
- ULGZDMOVFRHVEP-RWJQBGPGSA-N Erythromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)C(=O)[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 ULGZDMOVFRHVEP-RWJQBGPGSA-N 0.000 description 6
- 229930182566 Gentamicin Natural products 0.000 description 6
- CEAZRRDELHUEMR-URQXQFDESA-N Gentamicin Chemical compound O1[C@H](C(C)NC)CC[C@@H](N)[C@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H](NC)[C@@](C)(O)CO2)O)[C@H](N)C[C@@H]1N CEAZRRDELHUEMR-URQXQFDESA-N 0.000 description 6
- 206010063491 Herpes zoster oticus Diseases 0.000 description 6
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical compound C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 6
- 208000010315 Mastoiditis Diseases 0.000 description 6
- 108010003541 Platelet Activating Factor Proteins 0.000 description 6
- 208000032831 Ramsay Hunt syndrome Diseases 0.000 description 6
- 206010061373 Sudden Hearing Loss Diseases 0.000 description 6
- 206010047348 Vertigo positional Diseases 0.000 description 6
- 230000002159 abnormal effect Effects 0.000 description 6
- 230000001154 acute effect Effects 0.000 description 6
- 239000003429 antifungal agent Substances 0.000 description 6
- 239000000739 antihistaminic agent Substances 0.000 description 6
- 208000001870 benign paroxysmal positional vertigo Diseases 0.000 description 6
- BLFLLBZGZJTVJG-UHFFFAOYSA-N benzocaine Chemical compound CCOC(=O)C1=CC=C(N)C=C1 BLFLLBZGZJTVJG-UHFFFAOYSA-N 0.000 description 6
- 150000001557 benzodiazepines Chemical class 0.000 description 6
- 230000004071 biological effect Effects 0.000 description 6
- 230000015572 biosynthetic process Effects 0.000 description 6
- 230000015556 catabolic process Effects 0.000 description 6
- 230000008859 change Effects 0.000 description 6
- HVYWMOMLDIMFJA-DPAQBDIFSA-N cholesterol Chemical compound C1C=C2C[C@@H](O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@H]([C@H](C)CCCC(C)C)[C@@]1(C)CC2 HVYWMOMLDIMFJA-DPAQBDIFSA-N 0.000 description 6
- 210000003094 ear ossicle Anatomy 0.000 description 6
- 230000008029 eradication Effects 0.000 description 6
- 210000000256 facial nerve Anatomy 0.000 description 6
- 201000011349 geniculate herpes zoster Diseases 0.000 description 6
- 208000022760 infectious otitis media Diseases 0.000 description 6
- 230000028709 inflammatory response Effects 0.000 description 6
- 239000010410 layer Substances 0.000 description 6
- AGBQKNBQESQNJD-UHFFFAOYSA-N lipoic acid Chemical compound OC(=O)CCCCC1CCSS1 AGBQKNBQESQNJD-UHFFFAOYSA-N 0.000 description 6
- 230000003211 malignant effect Effects 0.000 description 6
- 229960001474 meclozine Drugs 0.000 description 6
- 210000002985 organ of corti Anatomy 0.000 description 6
- 206010033103 otosclerosis Diseases 0.000 description 6
- 230000037361 pathway Effects 0.000 description 6
- 230000002085 persistent effect Effects 0.000 description 6
- WIKYUJGCLQQFNW-UHFFFAOYSA-N prochlorperazine Chemical compound C1CN(C)CCN1CCCN1C2=CC(Cl)=CC=C2SC2=CC=CC=C21 WIKYUJGCLQQFNW-UHFFFAOYSA-N 0.000 description 6
- 230000000750 progressive effect Effects 0.000 description 6
- 235000018102 proteins Nutrition 0.000 description 6
- 102000004169 proteins and genes Human genes 0.000 description 6
- 230000002829 reductive effect Effects 0.000 description 6
- YGSDEFSMJLZEOE-UHFFFAOYSA-N salicylic acid Chemical compound OC(=O)C1=CC=CC=C1O YGSDEFSMJLZEOE-UHFFFAOYSA-N 0.000 description 6
- 235000015424 sodium Nutrition 0.000 description 6
- 229910052708 sodium Inorganic materials 0.000 description 6
- 229940083542 sodium Drugs 0.000 description 6
- 239000000243 solution Substances 0.000 description 6
- 208000006379 syphilis Diseases 0.000 description 6
- 230000000699 topical effect Effects 0.000 description 6
- 210000003273 vestibular nerve Anatomy 0.000 description 6
- 238000012800 visualization Methods 0.000 description 6
- 229930000680 A04AD01 - Scopolamine Natural products 0.000 description 5
- 102000003678 AMPA Receptors Human genes 0.000 description 5
- 108090000078 AMPA Receptors Proteins 0.000 description 5
- 102000004631 Calcineurin Human genes 0.000 description 5
- 108010042955 Calcineurin Proteins 0.000 description 5
- 206010010356 Congenital anomaly Diseases 0.000 description 5
- 206010014020 Ear pain Diseases 0.000 description 5
- 101150099612 Esrrb gene Proteins 0.000 description 5
- 206010017533 Fungal infection Diseases 0.000 description 5
- 208000007514 Herpes zoster Diseases 0.000 description 5
- STECJAGHUSJQJN-GAUPFVANSA-N Hyoscine Natural products C1([C@H](CO)C(=O)OC2C[C@@H]3N([C@H](C2)[C@@H]2[C@H]3O2)C)=CC=CC=C1 STECJAGHUSJQJN-GAUPFVANSA-N 0.000 description 5
- 206010020751 Hypersensitivity Diseases 0.000 description 5
- 206010020772 Hypertension Diseases 0.000 description 5
- 206010025421 Macule Diseases 0.000 description 5
- 208000031888 Mycoses Diseases 0.000 description 5
- STECJAGHUSJQJN-UHFFFAOYSA-N N-Methyl-scopolamin Natural products C1C(C2C3O2)N(C)C3CC1OC(=O)C(CO)C1=CC=CC=C1 STECJAGHUSJQJN-UHFFFAOYSA-N 0.000 description 5
- 229930193140 Neomycin Natural products 0.000 description 5
- 206010033101 Otorrhoea Diseases 0.000 description 5
- 241000283984 Rodentia Species 0.000 description 5
- 229940035676 analgesics Drugs 0.000 description 5
- 239000000730 antalgic agent Substances 0.000 description 5
- 201000000691 benign paroxysmal positional nystagmus Diseases 0.000 description 5
- 239000011575 calcium Substances 0.000 description 5
- 201000011510 cancer Diseases 0.000 description 5
- 238000007906 compression Methods 0.000 description 5
- 230000006835 compression Effects 0.000 description 5
- 230000003247 decreasing effect Effects 0.000 description 5
- 238000006731 degradation reaction Methods 0.000 description 5
- 239000003221 ear drop Substances 0.000 description 5
- 230000003492 excitotoxic effect Effects 0.000 description 5
- 231100000063 excitotoxicity Toxicity 0.000 description 5
- 230000014509 gene expression Effects 0.000 description 5
- 229960002518 gentamicin Drugs 0.000 description 5
- 235000010979 hydroxypropyl methyl cellulose Nutrition 0.000 description 5
- 229920003088 hydroxypropyl methyl cellulose Polymers 0.000 description 5
- 239000001866 hydroxypropyl methyl cellulose Substances 0.000 description 5
- UFVKGYZPFZQRLF-UHFFFAOYSA-N hydroxypropyl methyl cellulose Chemical compound OC1C(O)C(OC)OC(CO)C1OC1C(O)C(O)C(OC2C(C(O)C(OC3C(C(O)C(O)C(CO)O3)O)C(CO)O2)O)C(CO)O1 UFVKGYZPFZQRLF-UHFFFAOYSA-N 0.000 description 5
- 230000002757 inflammatory effect Effects 0.000 description 5
- 230000002401 inhibitory effect Effects 0.000 description 5
- 229940047122 interleukins Drugs 0.000 description 5
- 238000001990 intravenous administration Methods 0.000 description 5
- 239000003589 local anesthetic agent Substances 0.000 description 5
- 230000007774 longterm Effects 0.000 description 5
- 230000001404 mediated effect Effects 0.000 description 5
- 210000003470 mitochondria Anatomy 0.000 description 5
- 229960004927 neomycin Drugs 0.000 description 5
- 230000002842 otolith Effects 0.000 description 5
- 210000001265 otolithic membrane Anatomy 0.000 description 5
- 244000052769 pathogen Species 0.000 description 5
- 239000003755 preservative agent Substances 0.000 description 5
- 230000002265 prevention Effects 0.000 description 5
- 230000008569 process Effects 0.000 description 5
- 238000012545 processing Methods 0.000 description 5
- 229960003111 prochlorperazine Drugs 0.000 description 5
- 230000001105 regulatory effect Effects 0.000 description 5
- STECJAGHUSJQJN-FWXGHANASA-N scopolamine Chemical compound C1([C@@H](CO)C(=O)O[C@H]2C[C@@H]3N([C@H](C2)[C@@H]2[C@H]3O2)C)=CC=CC=C1 STECJAGHUSJQJN-FWXGHANASA-N 0.000 description 5
- 229960002646 scopolamine Drugs 0.000 description 5
- 238000013268 sustained release Methods 0.000 description 5
- 239000012730 sustained-release form Substances 0.000 description 5
- 210000000225 synapse Anatomy 0.000 description 5
- 231100000331 toxic Toxicity 0.000 description 5
- 230000002588 toxic effect Effects 0.000 description 5
- 238000012384 transportation and delivery Methods 0.000 description 5
- DIWRORZWFLOCLC-HNNXBMFYSA-N (3s)-7-chloro-5-(2-chlorophenyl)-3-hydroxy-1,3-dihydro-1,4-benzodiazepin-2-one Chemical compound N([C@H](C(NC1=CC=C(Cl)C=C11)=O)O)=C1C1=CC=CC=C1Cl DIWRORZWFLOCLC-HNNXBMFYSA-N 0.000 description 4
- RZVAJINKPMORJF-UHFFFAOYSA-N Acetaminophen Chemical compound CC(=O)NC1=CC=C(O)C=C1 RZVAJINKPMORJF-UHFFFAOYSA-N 0.000 description 4
- QMGUSPDJTPDFSF-UHFFFAOYSA-N Aldophosphamide Chemical compound ClCCN(CCCl)P(=O)(N)OCCC=O QMGUSPDJTPDFSF-UHFFFAOYSA-N 0.000 description 4
- 108010036221 Aquaporin 2 Proteins 0.000 description 4
- 102100034414 Aquaporin-2 Human genes 0.000 description 4
- 206010003694 Atrophy Diseases 0.000 description 4
- 208000010392 Bone Fractures Diseases 0.000 description 4
- VTYYLEPIZMXCLO-UHFFFAOYSA-L Calcium carbonate Chemical compound [Ca+2].[O-]C([O-])=O VTYYLEPIZMXCLO-UHFFFAOYSA-L 0.000 description 4
- 206010010904 Convulsion Diseases 0.000 description 4
- 108020004414 DNA Proteins 0.000 description 4
- AOJJSUZBOXZQNB-TZSSRYMLSA-N Doxorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 AOJJSUZBOXZQNB-TZSSRYMLSA-N 0.000 description 4
- 208000010201 Exanthema Diseases 0.000 description 4
- 241000233866 Fungi Species 0.000 description 4
- 108010072051 Glatiramer Acetate Proteins 0.000 description 4
- 206010019233 Headaches Diseases 0.000 description 4
- 208000001953 Hypotension Diseases 0.000 description 4
- HOKKHZGPKSLGJE-GSVOUGTGSA-N N-Methyl-D-aspartic acid Chemical compound CN[C@@H](C(O)=O)CC(O)=O HOKKHZGPKSLGJE-GSVOUGTGSA-N 0.000 description 4
- 102100022219 NF-kappa-B essential modulator Human genes 0.000 description 4
- 101710090077 NF-kappa-B essential modulator Proteins 0.000 description 4
- 108091000080 Phosphotransferase Proteins 0.000 description 4
- 206010035664 Pneumonia Diseases 0.000 description 4
- 239000002202 Polyethylene glycol Substances 0.000 description 4
- 239000004372 Polyvinyl alcohol Substances 0.000 description 4
- 208000003251 Pruritus Diseases 0.000 description 4
- 206010037660 Pyrexia Diseases 0.000 description 4
- LOUPRKONTZGTKE-WZBLMQSHSA-N Quinine Chemical compound C([C@H]([C@H](C1)C=C)C2)C[N@@]1[C@@H]2[C@H](O)C1=CC=NC2=CC=C(OC)C=C21 LOUPRKONTZGTKE-WZBLMQSHSA-N 0.000 description 4
- 206010040047 Sepsis Diseases 0.000 description 4
- 241000589970 Spirochaetales Species 0.000 description 4
- 239000004480 active ingredient Substances 0.000 description 4
- 239000000556 agonist Substances 0.000 description 4
- 229940125715 antihistaminic agent Drugs 0.000 description 4
- 230000037444 atrophy Effects 0.000 description 4
- 210000004369 blood Anatomy 0.000 description 4
- 239000008280 blood Substances 0.000 description 4
- 210000000170 cell membrane Anatomy 0.000 description 4
- 235000010980 cellulose Nutrition 0.000 description 4
- 210000001175 cerebrospinal fluid Anatomy 0.000 description 4
- 210000000262 cochlear duct Anatomy 0.000 description 4
- 229940038717 copaxone Drugs 0.000 description 4
- 210000003792 cranial nerve Anatomy 0.000 description 4
- 230000000254 damaging effect Effects 0.000 description 4
- UREBDLICKHMUKA-CXSFZGCWSA-N dexamethasone Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)CO)(O)[C@@]1(C)C[C@@H]2O UREBDLICKHMUKA-CXSFZGCWSA-N 0.000 description 4
- 238000009792 diffusion process Methods 0.000 description 4
- 239000002270 dispersing agent Substances 0.000 description 4
- 208000007176 earache Diseases 0.000 description 4
- 239000003792 electrolyte Substances 0.000 description 4
- 230000002708 enhancing effect Effects 0.000 description 4
- 201000005884 exanthem Diseases 0.000 description 4
- 238000013265 extended release Methods 0.000 description 4
- 230000012010 growth Effects 0.000 description 4
- 238000011554 guinea pig model Methods 0.000 description 4
- 231100000869 headache Toxicity 0.000 description 4
- 210000002216 heart Anatomy 0.000 description 4
- 230000036543 hypotension Effects 0.000 description 4
- 230000004941 influx Effects 0.000 description 4
- 230000002045 lasting effect Effects 0.000 description 4
- 210000003041 ligament Anatomy 0.000 description 4
- 230000000670 limiting effect Effects 0.000 description 4
- 229960004391 lorazepam Drugs 0.000 description 4
- 238000012423 maintenance Methods 0.000 description 4
- 201000006417 multiple sclerosis Diseases 0.000 description 4
- 230000001537 neural effect Effects 0.000 description 4
- 239000004031 partial agonist Substances 0.000 description 4
- 230000001717 pathogenic effect Effects 0.000 description 4
- 239000012071 phase Substances 0.000 description 4
- RJXQSIKBGKVNRT-UHFFFAOYSA-N phosphoramide mustard Chemical compound ClCCN(P(O)(=O)N)CCCl RJXQSIKBGKVNRT-UHFFFAOYSA-N 0.000 description 4
- 102000020233 phosphotransferase Human genes 0.000 description 4
- KASDHRXLYQOAKZ-ZPSXYTITSA-N pimecrolimus Chemical compound C/C([C@H]1OC(=O)[C@@H]2CCCCN2C(=O)C(=O)[C@]2(O)O[C@@H]([C@H](C[C@H]2C)OC)[C@@H](OC)C[C@@H](C)C/C(C)=C/[C@H](C(C[C@H](O)[C@H]1C)=O)CC)=C\[C@@H]1CC[C@@H](Cl)[C@H](OC)C1 KASDHRXLYQOAKZ-ZPSXYTITSA-N 0.000 description 4
- 229960005330 pimecrolimus Drugs 0.000 description 4
- 229920001983 poloxamer Polymers 0.000 description 4
- 229920001223 polyethylene glycol Polymers 0.000 description 4
- 229920000642 polymer Polymers 0.000 description 4
- 229940068984 polyvinyl alcohol Drugs 0.000 description 4
- 229920002451 polyvinyl alcohol Polymers 0.000 description 4
- 235000019422 polyvinyl alcohol Nutrition 0.000 description 4
- 230000001144 postural effect Effects 0.000 description 4
- 102000004196 processed proteins & peptides Human genes 0.000 description 4
- 108090000765 processed proteins & peptides Proteins 0.000 description 4
- 239000000047 product Substances 0.000 description 4
- 230000002035 prolonged effect Effects 0.000 description 4
- 206010037844 rash Diseases 0.000 description 4
- 210000001079 scala tympani Anatomy 0.000 description 4
- 230000028327 secretion Effects 0.000 description 4
- 230000035807 sensation Effects 0.000 description 4
- 230000003068 static effect Effects 0.000 description 4
- 229960005322 streptomycin Drugs 0.000 description 4
- 210000000645 stria vascularis Anatomy 0.000 description 4
- 239000004094 surface-active agent Substances 0.000 description 4
- 201000000596 systemic lupus erythematosus Diseases 0.000 description 4
- 238000013518 transcription Methods 0.000 description 4
- 230000035897 transcription Effects 0.000 description 4
- 238000011269 treatment regimen Methods 0.000 description 4
- URAYPUMNDPQOKB-UHFFFAOYSA-N triacetin Chemical compound CC(=O)OCC(OC(C)=O)COC(C)=O URAYPUMNDPQOKB-UHFFFAOYSA-N 0.000 description 4
- 229960004528 vincristine Drugs 0.000 description 4
- OGWKCGZFUXNPDA-XQKSVPLYSA-N vincristine Chemical compound C([N@]1C[C@@H](C[C@]2(C(=O)OC)C=3C(=CC4=C([C@]56[C@H]([C@@]([C@H](OC(C)=O)[C@]7(CC)C=CCN([C@H]67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)C[C@@](C1)(O)CC)CC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-XQKSVPLYSA-N 0.000 description 4
- OGWKCGZFUXNPDA-UHFFFAOYSA-N vincristine Natural products C1C(CC)(O)CC(CC2(C(=O)OC)C=3C(=CC4=C(C56C(C(C(OC(C)=O)C7(CC)C=CCN(C67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)CN1CCC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-UHFFFAOYSA-N 0.000 description 4
- RANONBLIHMVXAJ-UHFFFAOYSA-N 4-hydroxycyclophosphamide Chemical compound OC1CCOP(=O)(N(CCCl)CCCl)N1 RANONBLIHMVXAJ-UHFFFAOYSA-N 0.000 description 3
- NFLLKCVHYJRNRH-UHFFFAOYSA-N 8-chloro-1,3-dimethyl-7H-purine-2,6-dione 2-(diphenylmethyl)oxy-N,N-dimethylethanamine Chemical compound O=C1N(C)C(=O)N(C)C2=C1NC(Cl)=N2.C=1C=CC=CC=1C(OCCN(C)C)C1=CC=CC=C1 NFLLKCVHYJRNRH-UHFFFAOYSA-N 0.000 description 3
- QTBSBXVTEAMEQO-UHFFFAOYSA-N Acetic acid Chemical compound CC(O)=O QTBSBXVTEAMEQO-UHFFFAOYSA-N 0.000 description 3
- 206010002556 Ankylosing Spondylitis Diseases 0.000 description 3
- 208000009137 Behcet syndrome Diseases 0.000 description 3
- 108010006654 Bleomycin Proteins 0.000 description 3
- 229930186147 Cephalosporin Natural products 0.000 description 3
- 108091006146 Channels Proteins 0.000 description 3
- 206010008479 Chest Pain Diseases 0.000 description 3
- 208000032170 Congenital Abnormalities Diseases 0.000 description 3
- 208000034656 Contusions Diseases 0.000 description 3
- 208000000059 Dyspnea Diseases 0.000 description 3
- 206010013975 Dyspnoeas Diseases 0.000 description 3
- IAYPIBMASNFSPL-UHFFFAOYSA-N Ethylene oxide Chemical compound C1CO1 IAYPIBMASNFSPL-UHFFFAOYSA-N 0.000 description 3
- 208000004929 Facial Paralysis Diseases 0.000 description 3
- WSFSSNUMVMOOMR-UHFFFAOYSA-N Formaldehyde Chemical compound O=C WSFSSNUMVMOOMR-UHFFFAOYSA-N 0.000 description 3
- 102000005915 GABA Receptors Human genes 0.000 description 3
- 108010005551 GABA Receptors Proteins 0.000 description 3
- 208000032843 Hemorrhage Diseases 0.000 description 3
- 208000028782 Hereditary disease Diseases 0.000 description 3
- 108090001007 Interleukin-8 Proteins 0.000 description 3
- 102000004890 Interleukin-8 Human genes 0.000 description 3
- KFZMGEQAYNKOFK-UHFFFAOYSA-N Isopropanol Chemical compound CC(C)O KFZMGEQAYNKOFK-UHFFFAOYSA-N 0.000 description 3
- NNJVILVZKWQKPM-UHFFFAOYSA-N Lidocaine Chemical compound CCN(CC)CC(=O)NC1=C(C)C=CC=C1C NNJVILVZKWQKPM-UHFFFAOYSA-N 0.000 description 3
- 206010050551 Lupus-like syndrome Diseases 0.000 description 3
- 201000009906 Meningitis Diseases 0.000 description 3
- 241000699670 Mus sp. Species 0.000 description 3
- 206010061302 Myringitis Diseases 0.000 description 3
- 208000033212 Myringitis bullous Diseases 0.000 description 3
- 206010029240 Neuritis Diseases 0.000 description 3
- 206010033799 Paralysis Diseases 0.000 description 3
- 201000007100 Pharyngitis Diseases 0.000 description 3
- DNIAPMSPPWPWGF-UHFFFAOYSA-N Propylene glycol Chemical compound CC(O)CO DNIAPMSPPWPWGF-UHFFFAOYSA-N 0.000 description 3
- 102100036352 Protein disulfide-isomerase Human genes 0.000 description 3
- 241000193998 Streptococcus pneumoniae Species 0.000 description 3
- 208000036826 VIIth nerve paralysis Diseases 0.000 description 3
- 208000014070 Vestibular schwannoma Diseases 0.000 description 3
- 230000009102 absorption Effects 0.000 description 3
- 238000010521 absorption reaction Methods 0.000 description 3
- 208000004064 acoustic neuroma Diseases 0.000 description 3
- 239000002671 adjuvant Substances 0.000 description 3
- 230000032683 aging Effects 0.000 description 3
- 230000007815 allergy Effects 0.000 description 3
- 229960004821 amikacin Drugs 0.000 description 3
- LKCWBDHBTVXHDL-RMDFUYIESA-N amikacin Chemical compound O([C@@H]1[C@@H](N)C[C@H]([C@@H]([C@H]1O)O[C@@H]1[C@@H]([C@@H](N)[C@H](O)[C@@H](CO)O1)O)NC(=O)[C@@H](O)CCN)[C@H]1O[C@H](CN)[C@@H](O)[C@H](O)[C@H]1O LKCWBDHBTVXHDL-RMDFUYIESA-N 0.000 description 3
- 229940024606 amino acid Drugs 0.000 description 3
- 235000001014 amino acid Nutrition 0.000 description 3
- 150000001413 amino acids Chemical class 0.000 description 3
- 229960003022 amoxicillin Drugs 0.000 description 3
- LSQZJLSUYDQPKJ-NJBDSQKTSA-N amoxicillin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@H]3SC([C@@H](N3C2=O)C(O)=O)(C)C)=CC=C(O)C=C1 LSQZJLSUYDQPKJ-NJBDSQKTSA-N 0.000 description 3
- 229940121363 anti-inflammatory agent Drugs 0.000 description 3
- 239000002260 anti-inflammatory agent Substances 0.000 description 3
- 230000003110 anti-inflammatory effect Effects 0.000 description 3
- 230000006907 apoptotic process Effects 0.000 description 3
- 229960004099 azithromycin Drugs 0.000 description 3
- MQTOSJVFKKJCRP-BICOPXKESA-N azithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)N(C)C[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 MQTOSJVFKKJCRP-BICOPXKESA-N 0.000 description 3
- 210000003719 b-lymphocyte Anatomy 0.000 description 3
- 230000001580 bacterial effect Effects 0.000 description 3
- 244000052616 bacterial pathogen Species 0.000 description 3
- 229960005274 benzocaine Drugs 0.000 description 3
- 229960001561 bleomycin Drugs 0.000 description 3
- OYVAGSVQBOHSSS-UAPAGMARSA-O bleomycin A2 Chemical compound N([C@H](C(=O)N[C@H](C)[C@@H](O)[C@H](C)C(=O)N[C@@H]([C@H](O)C)C(=O)NCCC=1SC=C(N=1)C=1SC=C(N=1)C(=O)NCCC[S+](C)C)[C@@H](O[C@H]1[C@H]([C@@H](O)[C@H](O)[C@H](CO)O1)O[C@@H]1[C@H]([C@@H](OC(N)=O)[C@H](O)[C@@H](CO)O1)O)C=1N=CNC=1)C(=O)C1=NC([C@H](CC(N)=O)NC[C@H](N)C(N)=O)=NC(N)=C1C OYVAGSVQBOHSSS-UAPAGMARSA-O 0.000 description 3
- 229940046731 calcineurin inhibitors Drugs 0.000 description 3
- 239000012876 carrier material Substances 0.000 description 3
- 229960004755 ceftriaxone Drugs 0.000 description 3
- VAAUVRVFOQPIGI-SPQHTLEESA-N ceftriaxone Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC1=NC(=O)C(=O)NN1C VAAUVRVFOQPIGI-SPQHTLEESA-N 0.000 description 3
- 229940124587 cephalosporin Drugs 0.000 description 3
- 150000001780 cephalosporins Chemical class 0.000 description 3
- 239000013043 chemical agent Substances 0.000 description 3
- 238000006243 chemical reaction Methods 0.000 description 3
- 238000002512 chemotherapy Methods 0.000 description 3
- 235000012000 cholesterol Nutrition 0.000 description 3
- 230000002860 competitive effect Effects 0.000 description 3
- 238000002591 computed tomography Methods 0.000 description 3
- 208000027744 congestion Diseases 0.000 description 3
- 230000000875 corresponding effect Effects 0.000 description 3
- VQODGRNSFPNSQE-CXSFZGCWSA-N dexamethasone phosphate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)COP(O)(O)=O)(O)[C@@]1(C)C[C@@H]2O VQODGRNSFPNSQE-CXSFZGCWSA-N 0.000 description 3
- 229960002344 dexamethasone sodium phosphate Drugs 0.000 description 3
- 238000003745 diagnosis Methods 0.000 description 3
- AAOVKJBEBIDNHE-UHFFFAOYSA-N diazepam Chemical compound N=1CC(=O)N(C)C2=CC=C(Cl)C=C2C=1C1=CC=CC=C1 AAOVKJBEBIDNHE-UHFFFAOYSA-N 0.000 description 3
- 229960003529 diazepam Drugs 0.000 description 3
- 235000014113 dietary fatty acids Nutrition 0.000 description 3
- 239000002934 diuretic Substances 0.000 description 3
- 229940030606 diuretics Drugs 0.000 description 3
- 230000007613 environmental effect Effects 0.000 description 3
- 210000000981 epithelium Anatomy 0.000 description 3
- 229960003276 erythromycin Drugs 0.000 description 3
- 238000002474 experimental method Methods 0.000 description 3
- 206010016256 fatigue Diseases 0.000 description 3
- 229930195729 fatty acid Natural products 0.000 description 3
- 239000000194 fatty acid Substances 0.000 description 3
- 239000000835 fiber Substances 0.000 description 3
- 229960003692 gamma aminobutyric acid Drugs 0.000 description 3
- BTCSSZJGUNDROE-UHFFFAOYSA-N gamma-aminobutyric acid Chemical compound NCCCC(O)=O BTCSSZJGUNDROE-UHFFFAOYSA-N 0.000 description 3
- 229960001743 golimumab Drugs 0.000 description 3
- 230000009931 harmful effect Effects 0.000 description 3
- 210000002443 helper t lymphocyte Anatomy 0.000 description 3
- 230000001976 improved effect Effects 0.000 description 3
- 238000001727 in vivo Methods 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- 230000003993 interaction Effects 0.000 description 3
- 210000003734 kidney Anatomy 0.000 description 3
- 229960004194 lidocaine Drugs 0.000 description 3
- 235000019136 lipoic acid Nutrition 0.000 description 3
- 239000007788 liquid Substances 0.000 description 3
- 210000004185 liver Anatomy 0.000 description 3
- 238000002595 magnetic resonance imaging Methods 0.000 description 3
- 230000014759 maintenance of location Effects 0.000 description 3
- 210000001595 mastoid Anatomy 0.000 description 3
- 238000002483 medication Methods 0.000 description 3
- 230000028161 membrane depolarization Effects 0.000 description 3
- 230000002503 metabolic effect Effects 0.000 description 3
- 230000035772 mutation Effects 0.000 description 3
- 201000004237 myringitis bullosa hemorrhagica Diseases 0.000 description 3
- 210000004126 nerve fiber Anatomy 0.000 description 3
- 239000002858 neurotransmitter agent Substances 0.000 description 3
- 231100000252 nontoxic Toxicity 0.000 description 3
- 230000003000 nontoxic effect Effects 0.000 description 3
- 229950010444 onercept Drugs 0.000 description 3
- 230000001590 oxidative effect Effects 0.000 description 3
- LSQZJLSUYDQPKJ-UHFFFAOYSA-N p-Hydroxyampicillin Natural products O=C1N2C(C(O)=O)C(C)(C)SC2C1NC(=O)C(N)C1=CC=C(O)C=C1 LSQZJLSUYDQPKJ-UHFFFAOYSA-N 0.000 description 3
- FJKROLUGYXJWQN-UHFFFAOYSA-N papa-hydroxy-benzoic acid Natural products OC(=O)C1=CC=C(O)C=C1 FJKROLUGYXJWQN-UHFFFAOYSA-N 0.000 description 3
- 230000002093 peripheral effect Effects 0.000 description 3
- 230000026731 phosphorylation Effects 0.000 description 3
- 238000006366 phosphorylation reaction Methods 0.000 description 3
- 229920001184 polypeptide Polymers 0.000 description 3
- 229920000053 polysorbate 80 Polymers 0.000 description 3
- 229960005205 prednisolone Drugs 0.000 description 3
- OIGNJSKKLXVSLS-VWUMJDOOSA-N prednisolone Chemical compound O=C1C=C[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 OIGNJSKKLXVSLS-VWUMJDOOSA-N 0.000 description 3
- 229960004618 prednisone Drugs 0.000 description 3
- XOFYZVNMUHMLCC-ZPOLXVRWSA-N prednisone Chemical compound O=C1C=C[C@]2(C)[C@H]3C(=O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 XOFYZVNMUHMLCC-ZPOLXVRWSA-N 0.000 description 3
- 230000000770 proinflammatory effect Effects 0.000 description 3
- 230000000069 prophylactic effect Effects 0.000 description 3
- 108020003519 protein disulfide isomerase Proteins 0.000 description 3
- 230000000541 pulsatile effect Effects 0.000 description 3
- 238000001959 radiotherapy Methods 0.000 description 3
- 108010003189 recombinant human tumor necrosis factor-binding protein-1 Proteins 0.000 description 3
- CSYSULGPHGCBQD-UHFFFAOYSA-N s-ethylisothiouronium diethylphosphate Chemical compound CCSC(N)=N.CCOP(O)(=O)OCC CSYSULGPHGCBQD-UHFFFAOYSA-N 0.000 description 3
- 229960004889 salicylic acid Drugs 0.000 description 3
- 229940063122 sandimmune Drugs 0.000 description 3
- 210000001605 scala vestibuli Anatomy 0.000 description 3
- 210000000697 sensory organ Anatomy 0.000 description 3
- 230000011664 signaling Effects 0.000 description 3
- 210000003491 skin Anatomy 0.000 description 3
- 210000003625 skull Anatomy 0.000 description 3
- 239000003381 stabilizer Substances 0.000 description 3
- 230000002966 stenotic effect Effects 0.000 description 3
- 229940031000 streptococcus pneumoniae Drugs 0.000 description 3
- 238000011477 surgical intervention Methods 0.000 description 3
- 230000002459 sustained effect Effects 0.000 description 3
- 206010042772 syncope Diseases 0.000 description 3
- 210000002489 tectorial membrane Anatomy 0.000 description 3
- 229960002663 thioctic acid Drugs 0.000 description 3
- 210000001519 tissue Anatomy 0.000 description 3
- 229960000707 tobramycin Drugs 0.000 description 3
- NLVFBUXFDBBNBW-PBSUHMDJSA-S tobramycin(5+) Chemical compound [NH3+][C@@H]1C[C@H](O)[C@@H](C[NH3+])O[C@@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H]([NH3+])[C@H](O)[C@@H](CO)O2)O)[C@H]([NH3+])C[C@@H]1[NH3+] NLVFBUXFDBBNBW-PBSUHMDJSA-S 0.000 description 3
- 238000011200 topical administration Methods 0.000 description 3
- 238000012546 transfer Methods 0.000 description 3
- 210000000427 trigeminal ganglion Anatomy 0.000 description 3
- 201000008827 tuberculosis Diseases 0.000 description 3
- 208000025301 tympanitis Diseases 0.000 description 3
- QJVHTELASVOWBE-AGNWQMPPSA-N (2s,5r,6r)-6-[[(2r)-2-amino-2-(4-hydroxyphenyl)acetyl]amino]-3,3-dimethyl-7-oxo-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid;(2r,3z,5r)-3-(2-hydroxyethylidene)-7-oxo-4-oxa-1-azabicyclo[3.2.0]heptane-2-carboxylic acid Chemical compound OC(=O)[C@H]1C(=C/CO)/O[C@@H]2CC(=O)N21.C1([C@@H](N)C(=O)N[C@H]2[C@H]3SC([C@@H](N3C2=O)C(O)=O)(C)C)=CC=C(O)C=C1 QJVHTELASVOWBE-AGNWQMPPSA-N 0.000 description 2
- WDLWHQDACQUCJR-ZAMMOSSLSA-N (6r,7r)-7-[[(2r)-2-azaniumyl-2-(4-hydroxyphenyl)acetyl]amino]-8-oxo-3-[(e)-prop-1-enyl]-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)/C=C/C)C(O)=O)=CC=C(O)C=C1 WDLWHQDACQUCJR-ZAMMOSSLSA-N 0.000 description 2
- GPYKKBAAPVOCIW-HSASPSRMSA-N (6r,7s)-7-[[(2r)-2-amino-2-phenylacetyl]amino]-3-chloro-8-oxo-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid;hydrate Chemical compound O.C1([C@H](C(=O)N[C@@H]2C(N3C(=C(Cl)CC[C@@H]32)C(O)=O)=O)N)=CC=CC=C1 GPYKKBAAPVOCIW-HSASPSRMSA-N 0.000 description 2
- MGRVRXRGTBOSHW-UHFFFAOYSA-N (aminomethyl)phosphonic acid Chemical compound NCP(O)(O)=O MGRVRXRGTBOSHW-UHFFFAOYSA-N 0.000 description 2
- 230000006269 (delayed) early viral mRNA transcription Effects 0.000 description 2
- ZORQXIQZAOLNGE-UHFFFAOYSA-N 1,1-difluorocyclohexane Chemical compound FC1(F)CCCCC1 ZORQXIQZAOLNGE-UHFFFAOYSA-N 0.000 description 2
- GZGLPBNOIFLLRE-UHFFFAOYSA-N 1-[(5-methoxy-2-thiophen-2-ylquinazolin-4-yl)amino]-3-methylpyrrole-2,5-dione Chemical compound C=12C(OC)=CC=CC2=NC(C=2SC=CC=2)=NC=1NN1C(=O)C=C(C)C1=O GZGLPBNOIFLLRE-UHFFFAOYSA-N 0.000 description 2
- IXPNQXFRVYWDDI-UHFFFAOYSA-N 1-methyl-2,4-dioxo-1,3-diazinane-5-carboximidamide Chemical compound CN1CC(C(N)=N)C(=O)NC1=O IXPNQXFRVYWDDI-UHFFFAOYSA-N 0.000 description 2
- VBICKXHEKHSIBG-UHFFFAOYSA-N 1-monostearoylglycerol Chemical compound CCCCCCCCCCCCCCCCCC(=O)OCC(O)CO VBICKXHEKHSIBG-UHFFFAOYSA-N 0.000 description 2
- 208000004998 Abdominal Pain Diseases 0.000 description 2
- HGINCPLSRVDWNT-UHFFFAOYSA-N Acrolein Chemical compound C=CC=O HGINCPLSRVDWNT-UHFFFAOYSA-N 0.000 description 2
- 206010067484 Adverse reaction Diseases 0.000 description 2
- 201000004384 Alopecia Diseases 0.000 description 2
- CIWBSHSKHKDKBQ-JLAZNSOCSA-N Ascorbic acid Chemical compound OC[C@H](O)[C@H]1OC(=O)C(O)=C1O CIWBSHSKHKDKBQ-JLAZNSOCSA-N 0.000 description 2
- 241000228212 Aspergillus Species 0.000 description 2
- BSYNRYMUTXBXSQ-UHFFFAOYSA-N Aspirin Chemical compound CC(=O)OC1=CC=CC=C1C(O)=O BSYNRYMUTXBXSQ-UHFFFAOYSA-N 0.000 description 2
- COXVTLYNGOIATD-HVMBLDELSA-N CC1=C(C=CC(=C1)C1=CC(C)=C(C=C1)\N=N\C1=C(O)C2=C(N)C(=CC(=C2C=C1)S(O)(=O)=O)S(O)(=O)=O)\N=N\C1=CC=C2C(=CC(=C(N)C2=C1O)S(O)(=O)=O)S(O)(=O)=O Chemical compound CC1=C(C=CC(=C1)C1=CC(C)=C(C=C1)\N=N\C1=C(O)C2=C(N)C(=CC(=C2C=C1)S(O)(=O)=O)S(O)(=O)=O)\N=N\C1=CC=C2C(=CC(=C(N)C2=C1O)S(O)(=O)=O)S(O)(=O)=O COXVTLYNGOIATD-HVMBLDELSA-N 0.000 description 2
- 102000011727 Caspases Human genes 0.000 description 2
- 108010076667 Caspases Proteins 0.000 description 2
- 206010007882 Cellulitis Diseases 0.000 description 2
- 201000006082 Chickenpox Diseases 0.000 description 2
- 235000001258 Cinchona calisaya Nutrition 0.000 description 2
- 206010009900 Colitis ulcerative Diseases 0.000 description 2
- 208000000781 Conductive Hearing Loss Diseases 0.000 description 2
- 206010010280 Conductive deafness Diseases 0.000 description 2
- 229930105110 Cyclosporin A Natural products 0.000 description 2
- 241000701022 Cytomegalovirus Species 0.000 description 2
- 108010092160 Dactinomycin Proteins 0.000 description 2
- 206010051055 Deep vein thrombosis Diseases 0.000 description 2
- 208000016192 Demyelinating disease Diseases 0.000 description 2
- 206010015150 Erythema Diseases 0.000 description 2
- 206010063560 Excessive granulation tissue Diseases 0.000 description 2
- 206010056740 Genital discharge Diseases 0.000 description 2
- 102000018899 Glutamate Receptors Human genes 0.000 description 2
- 108010027915 Glutamate Receptors Proteins 0.000 description 2
- PEDCQBHIVMGVHV-UHFFFAOYSA-N Glycerine Chemical compound OCC(O)CO PEDCQBHIVMGVHV-UHFFFAOYSA-N 0.000 description 2
- 206010072579 Granulomatosis with polyangiitis Diseases 0.000 description 2
- 206010019196 Head injury Diseases 0.000 description 2
- 206010019280 Heart failures Diseases 0.000 description 2
- MHAJPDPJQMAIIY-UHFFFAOYSA-N Hydrogen peroxide Chemical compound OO MHAJPDPJQMAIIY-UHFFFAOYSA-N 0.000 description 2
- 229920002153 Hydroxypropyl cellulose Polymers 0.000 description 2
- 208000031226 Hyperlipidaemia Diseases 0.000 description 2
- HEFNNWSXXWATRW-UHFFFAOYSA-N Ibuprofen Chemical compound CC(C)CC1=CC=C(C(C)C(O)=O)C=C1 HEFNNWSXXWATRW-UHFFFAOYSA-N 0.000 description 2
- 206010062016 Immunosuppression Diseases 0.000 description 2
- 208000022559 Inflammatory bowel disease Diseases 0.000 description 2
- 206010022095 Injection Site reaction Diseases 0.000 description 2
- 102000006992 Interferon-alpha Human genes 0.000 description 2
- 108010047761 Interferon-alpha Proteins 0.000 description 2
- 102000003996 Interferon-beta Human genes 0.000 description 2
- 108090000467 Interferon-beta Proteins 0.000 description 2
- 108090001005 Interleukin-6 Proteins 0.000 description 2
- XEEYBQQBJWHFJM-UHFFFAOYSA-N Iron Chemical compound [Fe] XEEYBQQBJWHFJM-UHFFFAOYSA-N 0.000 description 2
- 208000035752 Live birth Diseases 0.000 description 2
- 102000004083 Lymphotoxin-alpha Human genes 0.000 description 2
- 108090000542 Lymphotoxin-alpha Proteins 0.000 description 2
- 241000878128 Malleus Species 0.000 description 2
- 241000124008 Mammalia Species 0.000 description 2
- 201000005505 Measles Diseases 0.000 description 2
- XUMBMVFBXHLACL-UHFFFAOYSA-N Melanin Chemical compound O=C1C(=O)C(C2=CNC3=C(C(C(=O)C4=C32)=O)C)=C2C4=CNC2=C1C XUMBMVFBXHLACL-UHFFFAOYSA-N 0.000 description 2
- 206010065838 Middle ear inflammation Diseases 0.000 description 2
- 108020005196 Mitochondrial DNA Proteins 0.000 description 2
- 208000005647 Mumps Diseases 0.000 description 2
- PSPFQEBFYXJZEV-UHFFFAOYSA-N N'-(1,8-dimethyl-4-imidazo[1,2-a]quinoxalinyl)ethane-1,2-diamine Chemical compound C1=C(C)C=C2N3C(C)=CN=C3C(NCCN)=NC2=C1 PSPFQEBFYXJZEV-UHFFFAOYSA-N 0.000 description 2
- LRHPLDYGYMQRHN-UHFFFAOYSA-N N-Butanol Chemical compound CCCCO LRHPLDYGYMQRHN-UHFFFAOYSA-N 0.000 description 2
- WHNWPMSKXPGLAX-UHFFFAOYSA-N N-Vinyl-2-pyrrolidone Chemical compound C=CN1CCCC1=O WHNWPMSKXPGLAX-UHFFFAOYSA-N 0.000 description 2
- 108010057466 NF-kappa B Proteins 0.000 description 2
- 102000003945 NF-kappa B Human genes 0.000 description 2
- 102000014736 Notch Human genes 0.000 description 2
- 208000003435 Optic Neuritis Diseases 0.000 description 2
- 206010068319 Oropharyngeal pain Diseases 0.000 description 2
- 208000005141 Otitis Diseases 0.000 description 2
- 206010033102 Otosalpingitis Diseases 0.000 description 2
- 206010033661 Pancytopenia Diseases 0.000 description 2
- RVGRUAULSDPKGF-UHFFFAOYSA-N Poloxamer Chemical compound C1CO1.CC1CO1 RVGRUAULSDPKGF-UHFFFAOYSA-N 0.000 description 2
- ZLMJMSJWJFRBEC-UHFFFAOYSA-N Potassium Chemical compound [K] ZLMJMSJWJFRBEC-UHFFFAOYSA-N 0.000 description 2
- 102000011383 Prestin Human genes 0.000 description 2
- 108050001617 Prestin Proteins 0.000 description 2
- GOOHAUXETOMSMM-UHFFFAOYSA-N Propylene oxide Chemical compound CC1CO1 GOOHAUXETOMSMM-UHFFFAOYSA-N 0.000 description 2
- 241000589517 Pseudomonas aeruginosa Species 0.000 description 2
- 206010057190 Respiratory tract infections Diseases 0.000 description 2
- NCYCYZXNIZJOKI-OVSJKPMPSA-N Retinaldehyde Chemical compound O=C\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C NCYCYZXNIZJOKI-OVSJKPMPSA-N 0.000 description 2
- CDMGBJANTYXAIV-UHFFFAOYSA-N SB 203580 Chemical compound C1=CC(S(=O)C)=CC=C1C1=NC(C=2C=CC(F)=CC=2)=C(C=2C=CN=CC=2)N1 CDMGBJANTYXAIV-UHFFFAOYSA-N 0.000 description 2
- GMBQZIIUCVWOCD-WWASVFFGSA-N Sarsapogenine Chemical compound O([C@@H]1[C@@H]([C@]2(CC[C@@H]3[C@@]4(C)CC[C@H](O)C[C@H]4CC[C@H]3[C@@H]2C1)C)[C@@H]1C)[C@]11CC[C@H](C)CO1 GMBQZIIUCVWOCD-WWASVFFGSA-N 0.000 description 2
- 206010039710 Scleroderma Diseases 0.000 description 2
- 206010040030 Sensory loss Diseases 0.000 description 2
- 208000021386 Sjogren Syndrome Diseases 0.000 description 2
- FAPWRFPIFSIZLT-UHFFFAOYSA-M Sodium chloride Chemical compound [Na+].[Cl-] FAPWRFPIFSIZLT-UHFFFAOYSA-M 0.000 description 2
- DBMJMQXJHONAFJ-UHFFFAOYSA-M Sodium laurylsulphate Chemical compound [Na+].CCCCCCCCCCCCOS([O-])(=O)=O DBMJMQXJHONAFJ-UHFFFAOYSA-M 0.000 description 2
- 241000191967 Staphylococcus aureus Species 0.000 description 2
- 208000006011 Stroke Diseases 0.000 description 2
- 210000001744 T-lymphocyte Anatomy 0.000 description 2
- 102000018679 Tacrolimus Binding Proteins Human genes 0.000 description 2
- 108010027179 Tacrolimus Binding Proteins Proteins 0.000 description 2
- AOBORMOPSGHCAX-UHFFFAOYSA-N Tocophersolan Chemical compound OCCOC(=O)CCC(=O)OC1=C(C)C(C)=C2OC(CCCC(C)CCCC(C)CCCC(C)C)(C)CCC2=C1C AOBORMOPSGHCAX-UHFFFAOYSA-N 0.000 description 2
- 241000589886 Treponema Species 0.000 description 2
- GLNADSQYFUSGOU-GPTZEZBUSA-J Trypan blue Chemical compound [Na+].[Na+].[Na+].[Na+].C1=C(S([O-])(=O)=O)C=C2C=C(S([O-])(=O)=O)C(/N=N/C3=CC=C(C=C3C)C=3C=C(C(=CC=3)\N=N\C=3C(=CC4=CC(=CC(N)=C4C=3O)S([O-])(=O)=O)S([O-])(=O)=O)C)=C(O)C2=C1N GLNADSQYFUSGOU-GPTZEZBUSA-J 0.000 description 2
- 201000006704 Ulcerative Colitis Diseases 0.000 description 2
- XSQUKJJJFZCRTK-UHFFFAOYSA-N Urea Chemical compound NC(N)=O XSQUKJJJFZCRTK-UHFFFAOYSA-N 0.000 description 2
- 108010059993 Vancomycin Proteins 0.000 description 2
- 206010046980 Varicella Diseases 0.000 description 2
- 206010047249 Venous thrombosis Diseases 0.000 description 2
- 230000005856 abnormality Effects 0.000 description 2
- DPXJVFZANSGRMM-UHFFFAOYSA-N acetic acid;2,3,4,5,6-pentahydroxyhexanal;sodium Chemical compound [Na].CC(O)=O.OCC(O)C(O)C(O)C(O)C=O DPXJVFZANSGRMM-UHFFFAOYSA-N 0.000 description 2
- 229960001138 acetylsalicylic acid Drugs 0.000 description 2
- 229960004150 aciclovir Drugs 0.000 description 2
- 229930183665 actinomycin Natural products 0.000 description 2
- 230000009471 action Effects 0.000 description 2
- 230000010398 acute inflammatory response Effects 0.000 description 2
- 230000006838 adverse reaction Effects 0.000 description 2
- 208000026935 allergic disease Diseases 0.000 description 2
- 230000003281 allosteric effect Effects 0.000 description 2
- 231100000360 alopecia Toxicity 0.000 description 2
- HRMVIAFZYCCHGF-BMCUWHFPSA-N am111 peptide Chemical compound C([C@H](C(=O)N[C@H](CC(C)C)C(=O)N[C@H](CC(N)=O)C(=O)N[C@H](CC(C)C)C(=O)N[C@H]([C@H](C)O)C(=O)N[C@H]([C@H](C)O)C(=O)N1[C@H](CCC1)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCCCN)C(=O)N1[C@H](CCC1)C(=O)N[C@H](CCCNC(N)=N)C(=O)N1[C@H](CCC1)C(=O)N1[C@H](CCC1)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCC(N)=O)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCCNC(N)=N)C(=O)N[C@H](CCCCN)C(=O)N[C@H](CCCCN)C(=O)N[C@H](CCCNC(N)=N)C(=O)NCC(O)=O)NC(=O)[C@@H]1N(CCC1)C(=O)[C@@H](CCC(N)=O)NC(=O)[C@H](NC(=O)[C@@H]1N(CCC1)C(=O)[C@@H](CCCNC(N)=N)NC(=O)[C@@H](CO)NC(=O)[C@@H](CCC(N)=O)NC(=O)[C@H](N)CC(O)=O)C(C)C)C1=CC=CC=C1 HRMVIAFZYCCHGF-BMCUWHFPSA-N 0.000 description 2
- 230000008485 antagonism Effects 0.000 description 2
- 230000002141 anti-parasite Effects 0.000 description 2
- 230000000842 anti-protozoal effect Effects 0.000 description 2
- 230000001754 anti-pyretic effect Effects 0.000 description 2
- 229940065524 anticholinergics inhalants for obstructive airway diseases Drugs 0.000 description 2
- 230000003078 antioxidant effect Effects 0.000 description 2
- 239000003096 antiparasitic agent Substances 0.000 description 2
- 239000003904 antiprotozoal agent Substances 0.000 description 2
- 239000002221 antipyretic Substances 0.000 description 2
- 229940125716 antipyretic agent Drugs 0.000 description 2
- 239000007864 aqueous solution Substances 0.000 description 2
- 206010003549 asthenia Diseases 0.000 description 2
- 210000003984 auditory pathway Anatomy 0.000 description 2
- VSRXQHXAPYXROS-UHFFFAOYSA-N azanide;cyclobutane-1,1-dicarboxylic acid;platinum(2+) Chemical compound [NH2-].[NH2-].[Pt+2].OC(=O)C1(C(O)=O)CCC1 VSRXQHXAPYXROS-UHFFFAOYSA-N 0.000 description 2
- 229940125717 barbiturate Drugs 0.000 description 2
- 238000005452 bending Methods 0.000 description 2
- BVGLIYRKPOITBQ-ANPZCEIESA-N benzylpenicillin benzathine Chemical compound C=1C=CC=CC=1C[NH2+]CC[NH2+]CC1=CC=CC=C1.N([C@H]1[C@H]2SC([C@@H](N2C1=O)C([O-])=O)(C)C)C(=O)CC1=CC=CC=C1.N([C@H]1[C@H]2SC([C@@H](N2C1=O)C([O-])=O)(C)C)C(=O)CC1=CC=CC=C1 BVGLIYRKPOITBQ-ANPZCEIESA-N 0.000 description 2
- 230000002146 bilateral effect Effects 0.000 description 2
- 239000003833 bile salt Substances 0.000 description 2
- 229940093761 bile salts Drugs 0.000 description 2
- 208000034158 bleeding Diseases 0.000 description 2
- 230000000740 bleeding effect Effects 0.000 description 2
- 230000017531 blood circulation Effects 0.000 description 2
- 210000001772 blood platelet Anatomy 0.000 description 2
- 210000004204 blood vessel Anatomy 0.000 description 2
- 239000001045 blue dye Substances 0.000 description 2
- 229960001467 bortezomib Drugs 0.000 description 2
- GXJABQQUPOEUTA-RDJZCZTQSA-N bortezomib Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)B(O)O)NC(=O)C=1N=CC=NC=1)C1=CC=CC=C1 GXJABQQUPOEUTA-RDJZCZTQSA-N 0.000 description 2
- 239000000872 buffer Substances 0.000 description 2
- 239000006227 byproduct Substances 0.000 description 2
- RYYVLZVUVIJVGH-UHFFFAOYSA-N caffeine Chemical compound CN1C(=O)N(C)C(=O)C2=C1N=CN2C RYYVLZVUVIJVGH-UHFFFAOYSA-N 0.000 description 2
- 229910000019 calcium carbonate Inorganic materials 0.000 description 2
- KVUAALJSMIVURS-ZEDZUCNESA-L calcium folinate Chemical compound [Ca+2].C1NC=2NC(N)=NC(=O)C=2N(C=O)C1CNC1=CC=C(C(=O)N[C@@H](CCC([O-])=O)C([O-])=O)C=C1 KVUAALJSMIVURS-ZEDZUCNESA-L 0.000 description 2
- YKPUWZUDDOIDPM-SOFGYWHQSA-N capsaicin Chemical compound COC1=CC(CNC(=O)CCCC\C=C\C(C)C)=CC=C1O YKPUWZUDDOIDPM-SOFGYWHQSA-N 0.000 description 2
- 239000002775 capsule Substances 0.000 description 2
- FFGPTBGBLSHEPO-UHFFFAOYSA-N carbamazepine Chemical compound C1=CC2=CC=CC=C2N(C(=O)N)C2=CC=CC=C21 FFGPTBGBLSHEPO-UHFFFAOYSA-N 0.000 description 2
- 229960004562 carboplatin Drugs 0.000 description 2
- 229940105329 carboxymethylcellulose Drugs 0.000 description 2
- LTINZAODLRIQIX-FBXRGJNPSA-N cefpodoxime proxetil Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC)C(=O)OC(C)OC(=O)OC(C)C)C(=O)C(=N/OC)\C1=CSC(N)=N1 LTINZAODLRIQIX-FBXRGJNPSA-N 0.000 description 2
- 229960004797 cefpodoxime proxetil Drugs 0.000 description 2
- 229960002580 cefprozil Drugs 0.000 description 2
- 230000003915 cell function Effects 0.000 description 2
- 239000003576 central nervous system agent Substances 0.000 description 2
- 229940125693 central nervous system agent Drugs 0.000 description 2
- 235000013339 cereals Nutrition 0.000 description 2
- 239000000812 cholinergic antagonist Substances 0.000 description 2
- 208000024035 chronic otitis media Diseases 0.000 description 2
- LOUPRKONTZGTKE-UHFFFAOYSA-N cinchonine Natural products C1C(C(C2)C=C)CCN2C1C(O)C1=CC=NC2=CC=C(OC)C=C21 LOUPRKONTZGTKE-UHFFFAOYSA-N 0.000 description 2
- MYSWGUAQZAJSOK-UHFFFAOYSA-N ciprofloxacin Chemical compound C12=CC(N3CCNCC3)=C(F)C=C2C(=O)C(C(=O)O)=CN1C1CC1 MYSWGUAQZAJSOK-UHFFFAOYSA-N 0.000 description 2
- 229960002626 clarithromycin Drugs 0.000 description 2
- AGOYDEPGAOXOCK-KCBOHYOISA-N clarithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)C(=O)[C@H](C)C[C@](C)([C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)OC)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 AGOYDEPGAOXOCK-KCBOHYOISA-N 0.000 description 2
- HZZVJAQRINQKSD-PBFISZAISA-N clavulanic acid Chemical compound OC(=O)[C@H]1C(=C/CO)/O[C@@H]2CC(=O)N21 HZZVJAQRINQKSD-PBFISZAISA-N 0.000 description 2
- 238000004891 communication Methods 0.000 description 2
- 208000023563 conductive hearing loss disease Diseases 0.000 description 2
- 230000001276 controlling effect Effects 0.000 description 2
- 230000036461 convulsion Effects 0.000 description 2
- 230000016396 cytokine production Effects 0.000 description 2
- 231100000895 deafness Toxicity 0.000 description 2
- 229940026692 decadron Drugs 0.000 description 2
- 230000007850 degeneration Effects 0.000 description 2
- 210000004443 dendritic cell Anatomy 0.000 description 2
- 230000001419 dependent effect Effects 0.000 description 2
- 230000006866 deterioration Effects 0.000 description 2
- 229960003957 dexamethasone Drugs 0.000 description 2
- 206010012601 diabetes mellitus Diseases 0.000 description 2
- JXTHNDFMNIQAHM-UHFFFAOYSA-N dichloroacetic acid Chemical compound OC(=O)C(Cl)Cl JXTHNDFMNIQAHM-UHFFFAOYSA-N 0.000 description 2
- 230000004069 differentiation Effects 0.000 description 2
- 229960004993 dimenhydrinate Drugs 0.000 description 2
- 231100000676 disease causative agent Toxicity 0.000 description 2
- 239000006185 dispersion Substances 0.000 description 2
- 238000001647 drug administration Methods 0.000 description 2
- 239000013583 drug formulation Substances 0.000 description 2
- 208000019258 ear infection Diseases 0.000 description 2
- 235000013601 eggs Nutrition 0.000 description 2
- 230000008030 elimination Effects 0.000 description 2
- 238000003379 elimination reaction Methods 0.000 description 2
- 229940073621 enbrel Drugs 0.000 description 2
- 210000001062 endolymphatic sac Anatomy 0.000 description 2
- 238000005516 engineering process Methods 0.000 description 2
- 210000002919 epithelial cell Anatomy 0.000 description 2
- 231100000321 erythema Toxicity 0.000 description 2
- AVOLMBLBETYQHX-UHFFFAOYSA-N etacrynic acid Chemical compound CCC(=C)C(=O)C1=CC=C(OCC(O)=O)C(Cl)=C1Cl AVOLMBLBETYQHX-UHFFFAOYSA-N 0.000 description 2
- 229960003699 evans blue Drugs 0.000 description 2
- 230000005713 exacerbation Effects 0.000 description 2
- 230000002964 excitative effect Effects 0.000 description 2
- 210000001508 eye Anatomy 0.000 description 2
- 150000004665 fatty acids Chemical class 0.000 description 2
- 108020001507 fusion proteins Proteins 0.000 description 2
- 102000037865 fusion proteins Human genes 0.000 description 2
- 239000007903 gelatin capsule Substances 0.000 description 2
- 229940062737 gengraf Drugs 0.000 description 2
- 239000001087 glyceryl triacetate Substances 0.000 description 2
- 235000013773 glyceryl triacetate Nutrition 0.000 description 2
- 210000001126 granulation tissue Anatomy 0.000 description 2
- 230000005484 gravity Effects 0.000 description 2
- 230000035876 healing Effects 0.000 description 2
- 231100000304 hepatotoxicity Toxicity 0.000 description 2
- 235000010977 hydroxypropyl cellulose Nutrition 0.000 description 2
- 229960001680 ibuprofen Drugs 0.000 description 2
- 210000002865 immune cell Anatomy 0.000 description 2
- 210000000987 immune system Anatomy 0.000 description 2
- 230000036039 immunity Effects 0.000 description 2
- 230000001506 immunosuppresive effect Effects 0.000 description 2
- 230000001771 impaired effect Effects 0.000 description 2
- 230000006872 improvement Effects 0.000 description 2
- 238000010348 incorporation Methods 0.000 description 2
- 210000001785 incus Anatomy 0.000 description 2
- 230000002458 infectious effect Effects 0.000 description 2
- 201000006747 infectious mononucleosis Diseases 0.000 description 2
- 206010022000 influenza Diseases 0.000 description 2
- 239000004615 ingredient Substances 0.000 description 2
- 230000000977 initiatory effect Effects 0.000 description 2
- 230000015788 innate immune response Effects 0.000 description 2
- 229940047124 interferons Drugs 0.000 description 2
- 238000007918 intramuscular administration Methods 0.000 description 2
- 229940125425 inverse agonist Drugs 0.000 description 2
- 230000007794 irritation Effects 0.000 description 2
- 208000028867 ischemia Diseases 0.000 description 2
- 230000007803 itching Effects 0.000 description 2
- 229960000318 kanamycin Drugs 0.000 description 2
- 229930027917 kanamycin Natural products 0.000 description 2
- SBUJHOSQTJFQJX-NOAMYHISSA-N kanamycin Chemical compound O[C@@H]1[C@@H](O)[C@H](O)[C@@H](CN)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H](N)[C@H](O)[C@@H](CO)O2)O)[C@H](N)C[C@@H]1N SBUJHOSQTJFQJX-NOAMYHISSA-N 0.000 description 2
- 229930182823 kanamycin A Natural products 0.000 description 2
- 150000002632 lipids Chemical class 0.000 description 2
- 229920006008 lipopolysaccharide Polymers 0.000 description 2
- 229960005015 local anesthetics Drugs 0.000 description 2
- 238000011866 long-term treatment Methods 0.000 description 2
- 239000002171 loop diuretic Substances 0.000 description 2
- 229960001977 loracarbef Drugs 0.000 description 2
- 208000018883 loss of balance Diseases 0.000 description 2
- 239000003120 macrolide antibiotic agent Substances 0.000 description 2
- 210000002540 macrophage Anatomy 0.000 description 2
- 239000011777 magnesium Substances 0.000 description 2
- 238000009115 maintenance therapy Methods 0.000 description 2
- 206010025482 malaise Diseases 0.000 description 2
- 210000002331 malleus Anatomy 0.000 description 2
- 230000004060 metabolic process Effects 0.000 description 2
- 208000022949 middle ear disease Diseases 0.000 description 2
- 208000010805 mumps infectious disease Diseases 0.000 description 2
- 210000003205 muscle Anatomy 0.000 description 2
- 230000004118 muscle contraction Effects 0.000 description 2
- 239000004081 narcotic agent Substances 0.000 description 2
- 201000009240 nasopharyngitis Diseases 0.000 description 2
- 230000002956 necrotizing effect Effects 0.000 description 2
- 229940063121 neoral Drugs 0.000 description 2
- 231100000417 nephrotoxicity Toxicity 0.000 description 2
- 230000007433 nerve pathway Effects 0.000 description 2
- 239000004090 neuroprotective agent Substances 0.000 description 2
- 230000001561 neurotransmitter reuptake Effects 0.000 description 2
- 230000007935 neutral effect Effects 0.000 description 2
- 208000004235 neutropenia Diseases 0.000 description 2
- 229940100688 oral solution Drugs 0.000 description 2
- 230000010355 oscillation Effects 0.000 description 2
- 230000003204 osmotic effect Effects 0.000 description 2
- 210000002997 osteoclast Anatomy 0.000 description 2
- NOOLISFMXDJSKH-UHFFFAOYSA-N p-menthan-3-ol Chemical compound CC(C)C1CCC(C)CC1O NOOLISFMXDJSKH-UHFFFAOYSA-N 0.000 description 2
- 229940124641 pain reliever Drugs 0.000 description 2
- 229960005489 paracetamol Drugs 0.000 description 2
- 208000035824 paresthesia Diseases 0.000 description 2
- 230000036961 partial effect Effects 0.000 description 2
- 235000019371 penicillin G benzathine Nutrition 0.000 description 2
- 230000008447 perception Effects 0.000 description 2
- 208000033808 peripheral neuropathy Diseases 0.000 description 2
- 230000003285 pharmacodynamic effect Effects 0.000 description 2
- WTJKGGKOPKCXLL-RRHRGVEJSA-N phosphatidylcholine Chemical compound CCCCCCCCCCCCCCCC(=O)OC[C@H](COP([O-])(=O)OCC[N+](C)(C)C)OC(=O)CCCCCCCC=CCCCCCCCC WTJKGGKOPKCXLL-RRHRGVEJSA-N 0.000 description 2
- 210000002381 plasma Anatomy 0.000 description 2
- 238000002616 plasmapheresis Methods 0.000 description 2
- 229920001992 poloxamer 407 Polymers 0.000 description 2
- 229920001987 poloxamine Polymers 0.000 description 2
- 235000010482 polyoxyethylene sorbitan monooleate Nutrition 0.000 description 2
- 239000000244 polyoxyethylene sorbitan monooleate Substances 0.000 description 2
- 229920001451 polypropylene glycol Polymers 0.000 description 2
- 229920000136 polysorbate Polymers 0.000 description 2
- 229940068968 polysorbate 80 Drugs 0.000 description 2
- 239000011591 potassium Substances 0.000 description 2
- 229910052700 potassium Inorganic materials 0.000 description 2
- 229910001414 potassium ion Inorganic materials 0.000 description 2
- 238000002360 preparation method Methods 0.000 description 2
- 230000010372 presbyacusis Effects 0.000 description 2
- 230000003449 preventive effect Effects 0.000 description 2
- DSKIOWHQLUWFLG-SPIKMXEPSA-N prochlorperazine maleate Chemical compound [H+].[H+].[H+].[H+].[O-]C(=O)\C=C/C([O-])=O.[O-]C(=O)\C=C/C([O-])=O.C1CN(C)CCN1CCCN1C2=CC(Cl)=CC=C2SC2=CC=CC=C21 DSKIOWHQLUWFLG-SPIKMXEPSA-N 0.000 description 2
- 229940072288 prograf Drugs 0.000 description 2
- 229960000948 quinine Drugs 0.000 description 2
- 239000000700 radioactive tracer Substances 0.000 description 2
- 208000020029 respiratory tract infectious disease Diseases 0.000 description 2
- 235000020945 retinal Nutrition 0.000 description 2
- 239000011604 retinal Substances 0.000 description 2
- 238000012552 review Methods 0.000 description 2
- 150000003902 salicylic acid esters Chemical class 0.000 description 2
- 230000002000 scavenging effect Effects 0.000 description 2
- 210000003949 semicircular duct Anatomy 0.000 description 2
- 230000035945 sensitivity Effects 0.000 description 2
- 208000024036 serous otitis media Diseases 0.000 description 2
- 201000009890 sinusitis Diseases 0.000 description 2
- 229940005550 sodium alginate Drugs 0.000 description 2
- 235000010413 sodium alginate Nutrition 0.000 description 2
- 239000000661 sodium alginate Substances 0.000 description 2
- 235000019812 sodium carboxymethyl cellulose Nutrition 0.000 description 2
- 229920001027 sodium carboxymethylcellulose Polymers 0.000 description 2
- 235000019333 sodium laurylsulphate Nutrition 0.000 description 2
- RMLUKZWYIKEASN-UHFFFAOYSA-M sodium;2-amino-9-(2-hydroxyethoxymethyl)purin-6-olate Chemical compound [Na+].O=C1[N-]C(N)=NC2=C1N=CN2COCCO RMLUKZWYIKEASN-UHFFFAOYSA-M 0.000 description 2
- 210000004872 soft tissue Anatomy 0.000 description 2
- 239000002904 solvent Substances 0.000 description 2
- 229940035049 sorbitan monooleate Drugs 0.000 description 2
- 235000011069 sorbitan monooleate Nutrition 0.000 description 2
- 239000001593 sorbitan monooleate Substances 0.000 description 2
- 241000894007 species Species 0.000 description 2
- 230000000638 stimulation Effects 0.000 description 2
- 230000035882 stress Effects 0.000 description 2
- 235000000346 sugar Nutrition 0.000 description 2
- 229940124530 sulfonamide Drugs 0.000 description 2
- 150000003456 sulfonamides Chemical class 0.000 description 2
- 238000012385 systemic delivery Methods 0.000 description 2
- 230000008685 targeting Effects 0.000 description 2
- 231100001274 therapeutic index Toxicity 0.000 description 2
- 239000003053 toxin Substances 0.000 description 2
- 108091008023 transcriptional regulators Proteins 0.000 description 2
- 230000001052 transient effect Effects 0.000 description 2
- 230000032258 transport Effects 0.000 description 2
- 208000009174 transverse myelitis Diseases 0.000 description 2
- 229960002622 triacetin Drugs 0.000 description 2
- 229940046728 tumor necrosis factor alpha inhibitor Drugs 0.000 description 2
- 239000002452 tumor necrosis factor alpha inhibitor Substances 0.000 description 2
- 108010072415 tumor necrosis factor precursor Proteins 0.000 description 2
- 229960003165 vancomycin Drugs 0.000 description 2
- MYPYJXKWCTUITO-LYRMYLQWSA-N vancomycin Chemical compound O([C@@H]1[C@@H](O)[C@H](O)[C@@H](CO)O[C@H]1OC1=C2C=C3C=C1OC1=CC=C(C=C1Cl)[C@@H](O)[C@H](C(N[C@@H](CC(N)=O)C(=O)N[C@H]3C(=O)N[C@H]1C(=O)N[C@H](C(N[C@@H](C3=CC(O)=CC(O)=C3C=3C(O)=CC=C1C=3)C(O)=O)=O)[C@H](O)C1=CC=C(C(=C1)Cl)O2)=O)NC(=O)[C@@H](CC(C)C)NC)[C@H]1C[C@](C)(N)[C@H](O)[C@H](C)O1 MYPYJXKWCTUITO-LYRMYLQWSA-N 0.000 description 2
- MYPYJXKWCTUITO-UHFFFAOYSA-N vancomycin Natural products O1C(C(=C2)Cl)=CC=C2C(O)C(C(NC(C2=CC(O)=CC(O)=C2C=2C(O)=CC=C3C=2)C(O)=O)=O)NC(=O)C3NC(=O)C2NC(=O)C(CC(N)=O)NC(=O)C(NC(=O)C(CC(C)C)NC)C(O)C(C=C3Cl)=CC=C3OC3=CC2=CC1=C3OC1OC(CO)C(O)C(O)C1OC1CC(C)(N)C(O)C(C)O1 MYPYJXKWCTUITO-UHFFFAOYSA-N 0.000 description 2
- NCYCYZXNIZJOKI-UHFFFAOYSA-N vitamin A aldehyde Natural products O=CC=C(C)C=CC=C(C)C=CC1=C(C)CCCC1(C)C NCYCYZXNIZJOKI-UHFFFAOYSA-N 0.000 description 2
- 239000000080 wetting agent Substances 0.000 description 2
- 229920001285 xanthan gum Polymers 0.000 description 2
- 229940124648 γ-Secretase Modulator Drugs 0.000 description 2
- AHOUBRCZNHFOSL-YOEHRIQHSA-N (+)-Casbol Chemical compound C1=CC(F)=CC=C1[C@H]1[C@H](COC=2C=C3OCOC3=CC=2)CNCC1 AHOUBRCZNHFOSL-YOEHRIQHSA-N 0.000 description 1
- AADVCYNFEREWOS-UHFFFAOYSA-N (+)-DDM Natural products C=CC=CC(C)C(OC(N)=O)C(C)C(O)C(C)CC(C)=CC(C)C(O)C(C)C=CC(O)CC1OC(=O)C(C)C(O)C1C AADVCYNFEREWOS-UHFFFAOYSA-N 0.000 description 1
- BMKDZUISNHGIBY-ZETCQYMHSA-N (+)-dexrazoxane Chemical compound C([C@H](C)N1CC(=O)NC(=O)C1)N1CC(=O)NC(=O)C1 BMKDZUISNHGIBY-ZETCQYMHSA-N 0.000 description 1
- SNICXCGAKADSCV-JTQLQIEISA-N (-)-Nicotine Chemical compound CN1CCC[C@H]1C1=CC=CN=C1 SNICXCGAKADSCV-JTQLQIEISA-N 0.000 description 1
- DQJCDTNMLBYVAY-ZXXIYAEKSA-N (2S,5R,10R,13R)-16-{[(2R,3S,4R,5R)-3-{[(2S,3R,4R,5S,6R)-3-acetamido-4,5-dihydroxy-6-(hydroxymethyl)oxan-2-yl]oxy}-5-(ethylamino)-6-hydroxy-2-(hydroxymethyl)oxan-4-yl]oxy}-5-(4-aminobutyl)-10-carbamoyl-2,13-dimethyl-4,7,12,15-tetraoxo-3,6,11,14-tetraazaheptadecan-1-oic acid Chemical class NCCCC[C@H](C(=O)N[C@@H](C)C(O)=O)NC(=O)CC[C@H](C(N)=O)NC(=O)[C@@H](C)NC(=O)C(C)O[C@@H]1[C@@H](NCC)C(O)O[C@H](CO)[C@H]1O[C@H]1[C@H](NC(C)=O)[C@@H](O)[C@H](O)[C@@H](CO)O1 DQJCDTNMLBYVAY-ZXXIYAEKSA-N 0.000 description 1
- WJTCHBVEUFDSIK-NWDGAFQWSA-N (2r,5s)-1-benzyl-2,5-dimethylpiperazine Chemical compound C[C@@H]1CN[C@@H](C)CN1CC1=CC=CC=C1 WJTCHBVEUFDSIK-NWDGAFQWSA-N 0.000 description 1
- KFSJYZYQSZKRRQ-BYPYZUCNSA-N (2s)-2-(hydroxyamino)-4-methylsulfanylbutanoic acid Chemical compound CSCC[C@H](NO)C(O)=O KFSJYZYQSZKRRQ-BYPYZUCNSA-N 0.000 description 1
- MIQJGZAEWQQAPN-YFKPBYRVSA-N (2s)-2-amino-4-methylsulfanylbutan-1-ol Chemical compound CSCC[C@H](N)CO MIQJGZAEWQQAPN-YFKPBYRVSA-N 0.000 description 1
- LOGFVTREOLYCPF-KXNHARMFSA-N (2s,3r)-2-[[(2r)-1-[(2s)-2,6-diaminohexanoyl]pyrrolidine-2-carbonyl]amino]-3-hydroxybutanoic acid Chemical compound C[C@@H](O)[C@@H](C(O)=O)NC(=O)[C@H]1CCCN1C(=O)[C@@H](N)CCCCN LOGFVTREOLYCPF-KXNHARMFSA-N 0.000 description 1
- VCOPTHOUUNAYKQ-WBTCAYNUSA-N (3s)-3,6-diamino-n-[[(2s,5s,8e,11s,15s)-15-amino-11-[(6r)-2-amino-1,4,5,6-tetrahydropyrimidin-6-yl]-8-[(carbamoylamino)methylidene]-2-(hydroxymethyl)-3,6,9,12,16-pentaoxo-1,4,7,10,13-pentazacyclohexadec-5-yl]methyl]hexanamide;(3s)-3,6-diamino-n-[[(2s,5s,8 Chemical compound N1C(=O)\C(=C/NC(N)=O)NC(=O)[C@H](CNC(=O)C[C@@H](N)CCCN)NC(=O)[C@H](C)NC(=O)[C@@H](N)CNC(=O)[C@@H]1[C@@H]1NC(N)=NCC1.N1C(=O)\C(=C/NC(N)=O)NC(=O)[C@H](CNC(=O)C[C@@H](N)CCCN)NC(=O)[C@H](CO)NC(=O)[C@@H](N)CNC(=O)[C@@H]1[C@@H]1NC(N)=NCC1 VCOPTHOUUNAYKQ-WBTCAYNUSA-N 0.000 description 1
- MEJYDZQQVZJMPP-ULAWRXDQSA-N (3s,3ar,6r,6ar)-3,6-dimethoxy-2,3,3a,5,6,6a-hexahydrofuro[3,2-b]furan Chemical compound CO[C@H]1CO[C@@H]2[C@H](OC)CO[C@@H]21 MEJYDZQQVZJMPP-ULAWRXDQSA-N 0.000 description 1
- VHNYOQKVZQVBLC-RTCGXNAVSA-N (4r,7e,9as)-7-[[3-methoxy-4-(4-methylimidazol-1-yl)phenyl]methylidene]-4-(3,4,5-trifluorophenyl)-1,3,4,8,9,9a-hexahydropyrido[2,1-c][1,4]oxazin-6-one Chemical compound C1([C@@H]2COC[C@@H]3CC\C(C(N32)=O)=C/C=2C=C(C(=CC=2)N2C=C(C)N=C2)OC)=CC(F)=C(F)C(F)=C1 VHNYOQKVZQVBLC-RTCGXNAVSA-N 0.000 description 1
- FPVKHBSQESCIEP-UHFFFAOYSA-N (8S)-3-(2-deoxy-beta-D-erythro-pentofuranosyl)-3,6,7,8-tetrahydroimidazo[4,5-d][1,3]diazepin-8-ol Natural products C1C(O)C(CO)OC1N1C(NC=NCC2O)=C2N=C1 FPVKHBSQESCIEP-UHFFFAOYSA-N 0.000 description 1
- FDKXTQMXEQVLRF-ZHACJKMWSA-N (E)-dacarbazine Chemical compound CN(C)\N=N\c1[nH]cnc1C(N)=O FDKXTQMXEQVLRF-ZHACJKMWSA-N 0.000 description 1
- CITHEXJVPOWHKC-UUWRZZSWSA-N 1,2-di-O-myristoyl-sn-glycero-3-phosphocholine Chemical compound CCCCCCCCCCCCCC(=O)OC[C@H](COP([O-])(=O)OCC[N+](C)(C)C)OC(=O)CCCCCCCCCCCCC CITHEXJVPOWHKC-UUWRZZSWSA-N 0.000 description 1
- LDVVTQMJQSCDMK-UHFFFAOYSA-N 1,3-dihydroxypropan-2-yl formate Chemical compound OCC(CO)OC=O LDVVTQMJQSCDMK-UHFFFAOYSA-N 0.000 description 1
- MQBZVUNNWUIPMK-UHFFFAOYSA-N 1-(2-bromophenyl)-3-(2-hydroxy-4-nitrophenyl)urea Chemical compound OC1=CC([N+]([O-])=O)=CC=C1NC(=O)NC1=CC=CC=C1Br MQBZVUNNWUIPMK-UHFFFAOYSA-N 0.000 description 1
- WDQFELCEOPFLCZ-UHFFFAOYSA-N 1-(2-hydroxyethyl)pyrrolidin-2-one Chemical compound OCCN1CCCC1=O WDQFELCEOPFLCZ-UHFFFAOYSA-N 0.000 description 1
- PZNPLUBHRSSFHT-RRHRGVEJSA-N 1-hexadecanoyl-2-octadecanoyl-sn-glycero-3-phosphocholine Chemical compound CCCCCCCCCCCCCCCCCC(=O)O[C@@H](COP([O-])(=O)OCC[N+](C)(C)C)COC(=O)CCCCCCCCCCCCCCC PZNPLUBHRSSFHT-RRHRGVEJSA-N 0.000 description 1
- VSNHCAURESNICA-NJFSPNSNSA-N 1-oxidanylurea Chemical compound N[14C](=O)NO VSNHCAURESNICA-NJFSPNSNSA-N 0.000 description 1
- WJFKNYWRSNBZNX-UHFFFAOYSA-N 10H-phenothiazine Chemical compound C1=CC=C2NC3=CC=CC=C3SC2=C1 WJFKNYWRSNBZNX-UHFFFAOYSA-N 0.000 description 1
- SVUOLADPCWQTTE-UHFFFAOYSA-N 1h-1,2-benzodiazepine Chemical compound N1N=CC=CC2=CC=CC=C12 SVUOLADPCWQTTE-UHFFFAOYSA-N 0.000 description 1
- NMIZONYLXCOHEF-UHFFFAOYSA-N 1h-imidazole-2-carboxamide Chemical compound NC(=O)C1=NC=CN1 NMIZONYLXCOHEF-UHFFFAOYSA-N 0.000 description 1
- QFWCYNPOPKQOKV-UHFFFAOYSA-N 2-(2-amino-3-methoxyphenyl)chromen-4-one Chemical compound COC1=CC=CC(C=2OC3=CC=CC=C3C(=O)C=2)=C1N QFWCYNPOPKQOKV-UHFFFAOYSA-N 0.000 description 1
- KZDCMKVLEYCGQX-UDPGNSCCSA-N 2-(diethylamino)ethyl 4-aminobenzoate;(2s,5r,6r)-3,3-dimethyl-7-oxo-6-[(2-phenylacetyl)amino]-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid;hydrate Chemical compound O.CCN(CC)CCOC(=O)C1=CC=C(N)C=C1.N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)CC1=CC=CC=C1 KZDCMKVLEYCGQX-UDPGNSCCSA-N 0.000 description 1
- CTPDSKVQLSDPLC-UHFFFAOYSA-N 2-(oxolan-2-ylmethoxy)ethanol Chemical compound OCCOCC1CCCO1 CTPDSKVQLSDPLC-UHFFFAOYSA-N 0.000 description 1
- VHVPQPYKVGDNFY-DFMJLFEVSA-N 2-[(2r)-butan-2-yl]-4-[4-[4-[4-[[(2r,4s)-2-(2,4-dichlorophenyl)-2-(1,2,4-triazol-1-ylmethyl)-1,3-dioxolan-4-yl]methoxy]phenyl]piperazin-1-yl]phenyl]-1,2,4-triazol-3-one Chemical compound O=C1N([C@H](C)CC)N=CN1C1=CC=C(N2CCN(CC2)C=2C=CC(OC[C@@H]3O[C@](CN4N=CN=C4)(OC3)C=3C(=CC(Cl)=CC=3)Cl)=CC=2)C=C1 VHVPQPYKVGDNFY-DFMJLFEVSA-N 0.000 description 1
- PBUUPFTVAPUWDE-UGZDLDLSSA-N 2-[[(2S,4S)-2-[bis(2-chloroethyl)amino]-2-oxo-1,3,2lambda5-oxazaphosphinan-4-yl]sulfanyl]ethanesulfonic acid Chemical compound OS(=O)(=O)CCS[C@H]1CCO[P@](=O)(N(CCCl)CCCl)N1 PBUUPFTVAPUWDE-UGZDLDLSSA-N 0.000 description 1
- SPCKHVPPRJWQRZ-UHFFFAOYSA-N 2-benzhydryloxy-n,n-dimethylethanamine;2-hydroxypropane-1,2,3-tricarboxylic acid Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O.C=1C=CC=CC=1C(OCCN(C)C)C1=CC=CC=C1 SPCKHVPPRJWQRZ-UHFFFAOYSA-N 0.000 description 1
- CLKJBNAGQKQOAV-UHFFFAOYSA-N 2-hydroxy-1,2-benzoselenazol-3-one Chemical compound C1=CC=CC2=C1[se]N(O)C2=O CLKJBNAGQKQOAV-UHFFFAOYSA-N 0.000 description 1
- RXIUEIPPLAFSDF-CYBMUJFWSA-N 2-hydroxy-n,n-dimethyl-3-[[2-[[(1r)-1-(5-methylfuran-2-yl)propyl]amino]-3,4-dioxocyclobuten-1-yl]amino]benzamide Chemical compound N([C@H](CC)C=1OC(C)=CC=1)C(C(C1=O)=O)=C1NC1=CC=CC(C(=O)N(C)C)=C1O RXIUEIPPLAFSDF-CYBMUJFWSA-N 0.000 description 1
- HZOABPDJUQEYFK-UHFFFAOYSA-N 2-methyl-n-[4-(1,2,3,4-tetrahydro-1,5-benzodiazepine-5-carbonyl)phenyl]benzamide Chemical compound CC1=CC=CC=C1C(=O)NC1=CC=C(C(=O)N2C3=CC=CC=C3NCCC2)C=C1 HZOABPDJUQEYFK-UHFFFAOYSA-N 0.000 description 1
- WZRJTRPJURQBRM-UHFFFAOYSA-N 4-amino-n-(5-methyl-1,2-oxazol-3-yl)benzenesulfonamide;5-[(3,4,5-trimethoxyphenyl)methyl]pyrimidine-2,4-diamine Chemical compound O1C(C)=CC(NS(=O)(=O)C=2C=CC(N)=CC=2)=N1.COC1=C(OC)C(OC)=CC(CC=2C(=NC(N)=NC=2)N)=C1 WZRJTRPJURQBRM-UHFFFAOYSA-N 0.000 description 1
- TVZGACDUOSZQKY-LBPRGKRZSA-N 4-aminofolic acid Chemical compound C1=NC2=NC(N)=NC(N)=C2N=C1CNC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 TVZGACDUOSZQKY-LBPRGKRZSA-N 0.000 description 1
- HIQIXEFWDLTDED-UHFFFAOYSA-N 4-hydroxy-1-piperidin-4-ylpyrrolidin-2-one Chemical compound O=C1CC(O)CN1C1CCNCC1 HIQIXEFWDLTDED-UHFFFAOYSA-N 0.000 description 1
- ISAVYTVYFVQUDY-UHFFFAOYSA-N 4-tert-Octylphenol Chemical compound CC(C)(C)CC(C)(C)C1=CC=C(O)C=C1 ISAVYTVYFVQUDY-UHFFFAOYSA-N 0.000 description 1
- IDPUKCWIGUEADI-UHFFFAOYSA-N 5-[bis(2-chloroethyl)amino]uracil Chemical compound ClCCN(CCCl)C1=CNC(=O)NC1=O IDPUKCWIGUEADI-UHFFFAOYSA-N 0.000 description 1
- XAUDJQYHKZQPEU-KVQBGUIXSA-N 5-aza-2'-deoxycytidine Chemical compound O=C1N=C(N)N=CN1[C@@H]1O[C@H](CO)[C@@H](O)C1 XAUDJQYHKZQPEU-KVQBGUIXSA-N 0.000 description 1
- YGUVFPOGHIKVPP-MUUNZHRXSA-N 6-(4-fluorophenyl)-n,n-dimethyl-3-[(3r)-3-pyridin-3-yl-1,3-dihydropyrrolo[1,2-c][1,3]thiazole-7-carbonyl]indole-1-carboxamide Chemical compound C1([C@@H]2N3C=CC(=C3CS2)C(=O)C2=CN(C3=CC(=CC=C32)C=2C=CC(F)=CC=2)C(=O)N(C)C)=CC=CN=C1 YGUVFPOGHIKVPP-MUUNZHRXSA-N 0.000 description 1
- WYWHKKSPHMUBEB-UHFFFAOYSA-N 6-Mercaptoguanine Natural products N1C(N)=NC(=S)C2=C1N=CN2 WYWHKKSPHMUBEB-UHFFFAOYSA-N 0.000 description 1
- XZIIFPSPUDAGJM-UHFFFAOYSA-N 6-chloro-2-n,2-n-diethylpyrimidine-2,4-diamine Polymers CCN(CC)C1=NC(N)=CC(Cl)=N1 XZIIFPSPUDAGJM-UHFFFAOYSA-N 0.000 description 1
- VVIAGPKUTFNRDU-UHFFFAOYSA-N 6S-folinic acid Natural products C1NC=2NC(N)=NC(=O)C=2N(C=O)C1CNC1=CC=C(C(=O)NC(CCC(O)=O)C(O)=O)C=C1 VVIAGPKUTFNRDU-UHFFFAOYSA-N 0.000 description 1
- FJHBVJOVLFPMQE-QFIPXVFZSA-N 7-Ethyl-10-Hydroxy-Camptothecin Chemical compound C1=C(O)C=C2C(CC)=C(CN3C(C4=C([C@@](C(=O)OC4)(O)CC)C=C33)=O)C3=NC2=C1 FJHBVJOVLFPMQE-QFIPXVFZSA-N 0.000 description 1
- GSDSWSVVBLHKDQ-UHFFFAOYSA-N 9-fluoro-3-methyl-10-(4-methylpiperazin-1-yl)-7-oxo-2,3-dihydro-7H-[1,4]oxazino[2,3,4-ij]quinoline-6-carboxylic acid Chemical compound FC1=CC(C(C(C(O)=O)=C2)=O)=C3N2C(C)COC3=C1N1CCN(C)CC1 GSDSWSVVBLHKDQ-UHFFFAOYSA-N 0.000 description 1
- 108010022579 ATP dependent 26S protease Proteins 0.000 description 1
- 230000002407 ATP formation Effects 0.000 description 1
- 206010060954 Abdominal Hernia Diseases 0.000 description 1
- 244000215068 Acacia senegal Species 0.000 description 1
- 235000006491 Acacia senegal Nutrition 0.000 description 1
- ZKHQWZAMYRWXGA-UHFFFAOYSA-N Adenosine triphosphate Natural products C1=NC=2C(N)=NC=NC=2N1C1OC(COP(O)(=O)OP(O)(=O)OP(O)(O)=O)C(O)C1O ZKHQWZAMYRWXGA-UHFFFAOYSA-N 0.000 description 1
- ZGCSNRKSJLVANE-UHFFFAOYSA-N Aglycone-Rebeccamycin Natural products N1C2=C3NC4=C(Cl)C=CC=C4C3=C(C(=O)NC3=O)C3=C2C2=C1C(Cl)=CC=C2 ZGCSNRKSJLVANE-UHFFFAOYSA-N 0.000 description 1
- 102000002260 Alkaline Phosphatase Human genes 0.000 description 1
- 108020004774 Alkaline Phosphatase Proteins 0.000 description 1
- 206010002198 Anaphylactic reaction Diseases 0.000 description 1
- 241000252073 Anguilliformes Species 0.000 description 1
- 206010002961 Aplasia Diseases 0.000 description 1
- 208000032467 Aplastic anaemia Diseases 0.000 description 1
- 101100515517 Arabidopsis thaliana XI-I gene Proteins 0.000 description 1
- 206010053555 Arthritis bacterial Diseases 0.000 description 1
- 241000416162 Astragalus gummifer Species 0.000 description 1
- 206010003598 Atelectasis Diseases 0.000 description 1
- 201000001320 Atherosclerosis Diseases 0.000 description 1
- 206010003658 Atrial Fibrillation Diseases 0.000 description 1
- 208000008035 Back Pain Diseases 0.000 description 1
- KPYSYYIEGFHWSV-UHFFFAOYSA-N Baclofen Chemical compound OC(=O)CC(CN)C1=CC=C(Cl)C=C1 KPYSYYIEGFHWSV-UHFFFAOYSA-N 0.000 description 1
- 206010058460 Bacterial labyrinthitis Diseases 0.000 description 1
- WVDDGKGOMKODPV-UHFFFAOYSA-N Benzyl alcohol Chemical compound OCC1=CC=CC=C1 WVDDGKGOMKODPV-UHFFFAOYSA-N 0.000 description 1
- 208000019838 Blood disease Diseases 0.000 description 1
- 241000589968 Borrelia Species 0.000 description 1
- 208000002381 Brain Hypoxia Diseases 0.000 description 1
- 201000006474 Brain Ischemia Diseases 0.000 description 1
- 208000003174 Brain Neoplasms Diseases 0.000 description 1
- 208000014644 Brain disease Diseases 0.000 description 1
- 102000004219 Brain-derived neurotrophic factor Human genes 0.000 description 1
- 108090000715 Brain-derived neurotrophic factor Proteins 0.000 description 1
- SGHZXLIDFTYFHQ-UHFFFAOYSA-L Brilliant Blue Chemical compound [Na+].[Na+].C=1C=C(C(=C2C=CC(C=C2)=[N+](CC)CC=2C=C(C=CC=2)S([O-])(=O)=O)C=2C(=CC=CC=2)S([O-])(=O)=O)C=CC=1N(CC)CC1=CC=CC(S([O-])(=O)=O)=C1 SGHZXLIDFTYFHQ-UHFFFAOYSA-L 0.000 description 1
- 241001598984 Bromius obscurus Species 0.000 description 1
- 208000009079 Bronchial Spasm Diseases 0.000 description 1
- 208000014181 Bronchial disease Diseases 0.000 description 1
- 206010006482 Bronchospasm Diseases 0.000 description 1
- 206010006784 Burning sensation Diseases 0.000 description 1
- 206010006811 Bursitis Diseases 0.000 description 1
- COVZYZSDYWQREU-UHFFFAOYSA-N Busulfan Chemical compound CS(=O)(=O)OCCCCOS(C)(=O)=O COVZYZSDYWQREU-UHFFFAOYSA-N 0.000 description 1
- NLZUEZXRPGMBCV-UHFFFAOYSA-N Butylhydroxytoluene Chemical compound CC1=CC(C(C)(C)C)=C(O)C(C(C)(C)C)=C1 NLZUEZXRPGMBCV-UHFFFAOYSA-N 0.000 description 1
- 102100028989 C-X-C chemokine receptor type 2 Human genes 0.000 description 1
- 229960005509 CAT-3888 Drugs 0.000 description 1
- 229960005529 CRLX101 Drugs 0.000 description 1
- OYPRJOBELJOOCE-UHFFFAOYSA-N Calcium Chemical compound [Ca] OYPRJOBELJOOCE-UHFFFAOYSA-N 0.000 description 1
- 239000001736 Calcium glycerylphosphate Substances 0.000 description 1
- KLWPJMFMVPTNCC-UHFFFAOYSA-N Camptothecin Natural products CCC1(O)C(=O)OCC2=C1C=C3C4Nc5ccccc5C=C4CN3C2=O KLWPJMFMVPTNCC-UHFFFAOYSA-N 0.000 description 1
- 241000222122 Candida albicans Species 0.000 description 1
- GAGWJHPBXLXJQN-UORFTKCHSA-N Capecitabine Chemical compound C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1[C@H]1[C@H](O)[C@H](O)[C@@H](C)O1 GAGWJHPBXLXJQN-UORFTKCHSA-N 0.000 description 1
- GAGWJHPBXLXJQN-UHFFFAOYSA-N Capecitabine Natural products C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1C1C(O)C(O)C(C)O1 GAGWJHPBXLXJQN-UHFFFAOYSA-N 0.000 description 1
- 108010065839 Capreomycin Proteins 0.000 description 1
- BVKZGUZCCUSVTD-UHFFFAOYSA-L Carbonate Chemical compound [O-]C([O-])=O BVKZGUZCCUSVTD-UHFFFAOYSA-L 0.000 description 1
- 201000009030 Carcinoma Diseases 0.000 description 1
- 206010007559 Cardiac failure congestive Diseases 0.000 description 1
- 206010048610 Cardiotoxicity Diseases 0.000 description 1
- 208000024172 Cardiovascular disease Diseases 0.000 description 1
- 108010078791 Carrier Proteins Proteins 0.000 description 1
- 102000000844 Cell Surface Receptors Human genes 0.000 description 1
- 108010001857 Cell Surface Receptors Proteins 0.000 description 1
- 206010008120 Cerebral ischaemia Diseases 0.000 description 1
- 206010050337 Cerumen impaction Diseases 0.000 description 1
- 229920001661 Chitosan Polymers 0.000 description 1
- JWBOIMRXGHLCPP-UHFFFAOYSA-N Chloditan Chemical compound C=1C=CC=C(Cl)C=1C(C(Cl)Cl)C1=CC=C(Cl)C=C1 JWBOIMRXGHLCPP-UHFFFAOYSA-N 0.000 description 1
- VEXZGXHMUGYJMC-UHFFFAOYSA-M Chloride anion Chemical compound [Cl-] VEXZGXHMUGYJMC-UHFFFAOYSA-M 0.000 description 1
- 108010009685 Cholinergic Receptors Proteins 0.000 description 1
- VYZAMTAEIAYCRO-UHFFFAOYSA-N Chromium Chemical compound [Cr] VYZAMTAEIAYCRO-UHFFFAOYSA-N 0.000 description 1
- 208000030939 Chronic inflammatory demyelinating polyneuropathy Diseases 0.000 description 1
- PTOAARAWEBMLNO-KVQBGUIXSA-N Cladribine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@H]1C[C@H](O)[C@@H](CO)O1 PTOAARAWEBMLNO-KVQBGUIXSA-N 0.000 description 1
- 208000010007 Cogan syndrome Diseases 0.000 description 1
- 208000028698 Cognitive impairment Diseases 0.000 description 1
- 206010010264 Condition aggravated Diseases 0.000 description 1
- 206010010774 Constipation Diseases 0.000 description 1
- 229920000742 Cotton Polymers 0.000 description 1
- 206010011224 Cough Diseases 0.000 description 1
- 108010069514 Cyclic Peptides Proteins 0.000 description 1
- 102000001189 Cyclic Peptides Human genes 0.000 description 1
- 229920000858 Cyclodextrin Polymers 0.000 description 1
- 102000001493 Cyclophilins Human genes 0.000 description 1
- 108010068682 Cyclophilins Proteins 0.000 description 1
- 108010036941 Cyclosporins Proteins 0.000 description 1
- 206010011732 Cyst Diseases 0.000 description 1
- 206010011793 Cystitis haemorrhagic Diseases 0.000 description 1
- UHDGCWIWMRVCDJ-CCXZUQQUSA-N Cytarabine Chemical compound O=C1N=C(N)C=CN1[C@H]1[C@@H](O)[C@H](O)[C@@H](CO)O1 UHDGCWIWMRVCDJ-CCXZUQQUSA-N 0.000 description 1
- 208000004449 DNA Virus Infections Diseases 0.000 description 1
- ZBNZXTGUTAYRHI-UHFFFAOYSA-N Dasatinib Chemical compound C=1C(N2CCN(CCO)CC2)=NC(C)=NC=1NC(S1)=NC=C1C(=O)NC1=C(C)C=CC=C1Cl ZBNZXTGUTAYRHI-UHFFFAOYSA-N 0.000 description 1
- 206010061619 Deformity Diseases 0.000 description 1
- 208000019505 Deglutition disease Diseases 0.000 description 1
- 201000004624 Dermatitis Diseases 0.000 description 1
- 206010012438 Dermatitis atopic Diseases 0.000 description 1
- 206010051392 Diapedesis Diseases 0.000 description 1
- 206010012713 Diaphragmatic hernia Diseases 0.000 description 1
- 206010012735 Diarrhoea Diseases 0.000 description 1
- MYMOFIZGZYHOMD-UHFFFAOYSA-N Dioxygen Chemical compound O=O MYMOFIZGZYHOMD-UHFFFAOYSA-N 0.000 description 1
- AADVCYNFEREWOS-OBRABYBLSA-N Discodermolide Chemical compound C=C\C=C/[C@H](C)[C@H](OC(N)=O)[C@@H](C)[C@H](O)[C@@H](C)C\C(C)=C/[C@H](C)[C@@H](O)[C@@H](C)\C=C/[C@@H](O)C[C@@H]1OC(=O)[C@H](C)[C@@H](O)[C@H]1C AADVCYNFEREWOS-OBRABYBLSA-N 0.000 description 1
- 208000003556 Dry Eye Syndromes Diseases 0.000 description 1
- 206010013774 Dry eye Diseases 0.000 description 1
- 229920005682 EO-PO block copolymer Polymers 0.000 description 1
- 206010014016 Ear malformation Diseases 0.000 description 1
- 206010014025 Ear swelling Diseases 0.000 description 1
- DYEFUKCXAQOFHX-UHFFFAOYSA-N Ebselen Chemical compound [se]1C2=CC=CC=C2C(=O)N1C1=CC=CC=C1 DYEFUKCXAQOFHX-UHFFFAOYSA-N 0.000 description 1
- XXPXYPLPSDPERN-UHFFFAOYSA-N Ecteinascidin 743 Natural products COc1cc2C(NCCc2cc1O)C(=O)OCC3N4C(O)C5Cc6cc(C)c(OC)c(O)c6C(C4C(S)c7c(OC(=O)C)c(C)c8OCOc8c37)N5C XXPXYPLPSDPERN-UHFFFAOYSA-N 0.000 description 1
- LVGKNOAMLMIIKO-UHFFFAOYSA-N Elaidinsaeure-aethylester Natural products CCCCCCCCC=CCCCCCCCC(=O)OCC LVGKNOAMLMIIKO-UHFFFAOYSA-N 0.000 description 1
- 206010014418 Electrolyte imbalance Diseases 0.000 description 1
- 208000032274 Encephalopathy Diseases 0.000 description 1
- 201000000297 Erysipelas Diseases 0.000 description 1
- LFQSCWFLJHTTHZ-UHFFFAOYSA-N Ethanol Chemical compound CCO LFQSCWFLJHTTHZ-UHFFFAOYSA-N 0.000 description 1
- HKVAMNSJSFKALM-GKUWKFKPSA-N Everolimus Chemical compound C1C[C@@H](OCCO)[C@H](OC)C[C@@H]1C[C@@H](C)[C@H]1OC(=O)[C@@H]2CCCCN2C(=O)C(=O)[C@](O)(O2)[C@H](C)CC[C@H]2C[C@H](OC)/C(C)=C/C=C/C=C/[C@@H](C)C[C@@H](C)C(=O)[C@H](OC)[C@H](O)/C(C)=C/[C@@H](C)C(=O)C1 HKVAMNSJSFKALM-GKUWKFKPSA-N 0.000 description 1
- 208000009386 Experimental Arthritis Diseases 0.000 description 1
- 206010063602 Exposure to noise Diseases 0.000 description 1
- 108010089357 FR 235222 Proteins 0.000 description 1
- 239000004214 Fast Green FCF Substances 0.000 description 1
- 206010053172 Fatal outcomes Diseases 0.000 description 1
- 206010016717 Fistula Diseases 0.000 description 1
- 206010051283 Fluid imbalance Diseases 0.000 description 1
- KRHYYFGTRYWZRS-UHFFFAOYSA-M Fluoride anion Chemical compound [F-] KRHYYFGTRYWZRS-UHFFFAOYSA-M 0.000 description 1
- GHASVSINZRGABV-UHFFFAOYSA-N Fluorouracil Chemical compound FC1=CNC(=O)NC1=O GHASVSINZRGABV-UHFFFAOYSA-N 0.000 description 1
- YPINZEGNLULHHT-UHFFFAOYSA-N Fujimycin Natural products COC1CC(CCC1O)C=C(/C)C2OC(=O)C3CCCCCN3C(=O)C(=O)C4(O)OC(C(CC4C)OC)C(OC)C(C)CC(=CC(CC=C)C(=O)CC(O)C2C)C YPINZEGNLULHHT-UHFFFAOYSA-N 0.000 description 1
- 229910052688 Gadolinium Inorganic materials 0.000 description 1
- 208000007882 Gastritis Diseases 0.000 description 1
- 208000005577 Gastroenteritis Diseases 0.000 description 1
- 208000012671 Gastrointestinal haemorrhages Diseases 0.000 description 1
- 241000237858 Gastropoda Species 0.000 description 1
- 108010010803 Gelatin Proteins 0.000 description 1
- 101001070329 Geobacillus stearothermophilus 50S ribosomal protein L18 Proteins 0.000 description 1
- 102000034575 Glutamate transporters Human genes 0.000 description 1
- 108091006151 Glutamate transporters Proteins 0.000 description 1
- 229920002907 Guar gum Polymers 0.000 description 1
- 208000035895 Guillain-Barré syndrome Diseases 0.000 description 1
- 229920000084 Gum arabic Polymers 0.000 description 1
- 229920003114 HPC-L Polymers 0.000 description 1
- 229920003115 HPC-SL Polymers 0.000 description 1
- 208000032041 Hearing impaired Diseases 0.000 description 1
- 208000010496 Heart Arrest Diseases 0.000 description 1
- 206010019851 Hepatotoxicity Diseases 0.000 description 1
- 208000009889 Herpes Simplex Diseases 0.000 description 1
- 241000228402 Histoplasma Species 0.000 description 1
- 201000002563 Histoplasmosis Diseases 0.000 description 1
- 101000599951 Homo sapiens Insulin-like growth factor I Proteins 0.000 description 1
- 101001076422 Homo sapiens Interleukin-1 receptor type 2 Proteins 0.000 description 1
- 101001055144 Homo sapiens Interleukin-2 receptor subunit alpha Proteins 0.000 description 1
- 101001055222 Homo sapiens Interleukin-8 Proteins 0.000 description 1
- 229920000663 Hydroxyethyl cellulose Polymers 0.000 description 1
- 239000004354 Hydroxyethyl cellulose Substances 0.000 description 1
- 208000035150 Hypercholesterolemia Diseases 0.000 description 1
- 208000010086 Hypertelorism Diseases 0.000 description 1
- 206010020771 Hypertelorism of orbit Diseases 0.000 description 1
- 208000004044 Hypesthesia Diseases 0.000 description 1
- XDXDZDZNSLXDNA-UHFFFAOYSA-N Idarubicin Natural products C1C(N)C(O)C(C)OC1OC1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2CC(O)(C(C)=O)C1 XDXDZDZNSLXDNA-UHFFFAOYSA-N 0.000 description 1
- XDXDZDZNSLXDNA-TZNDIEGXSA-N Idarubicin Chemical compound C1[C@H](N)[C@H](O)[C@H](C)O[C@H]1O[C@@H]1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2C[C@@](O)(C(C)=O)C1 XDXDZDZNSLXDNA-TZNDIEGXSA-N 0.000 description 1
- 206010021403 Illusion Diseases 0.000 description 1
- 102000000521 Immunophilins Human genes 0.000 description 1
- 108010016648 Immunophilins Proteins 0.000 description 1
- 208000026350 Inborn Genetic disease Diseases 0.000 description 1
- 208000004575 Infectious Arthritis Diseases 0.000 description 1
- 206010022052 Injection site bruising Diseases 0.000 description 1
- 206010022067 Injection site haemorrhage Diseases 0.000 description 1
- 108090000723 Insulin-Like Growth Factor I Proteins 0.000 description 1
- 102000004218 Insulin-Like Growth Factor I Human genes 0.000 description 1
- 102100037852 Insulin-like growth factor I Human genes 0.000 description 1
- 229940124084 Interleukin 1 antagonist Drugs 0.000 description 1
- 102000003777 Interleukin-1 beta Human genes 0.000 description 1
- 108090000193 Interleukin-1 beta Proteins 0.000 description 1
- 102100026017 Interleukin-1 receptor type 2 Human genes 0.000 description 1
- 108090000978 Interleukin-4 Proteins 0.000 description 1
- 102100026236 Interleukin-8 Human genes 0.000 description 1
- 108010018951 Interleukin-8B Receptors Proteins 0.000 description 1
- LPHGQDQBBGAPDZ-UHFFFAOYSA-N Isocaffeine Natural products CN1C(=O)N(C)C(=O)C2=C1N(C)C=N2 LPHGQDQBBGAPDZ-UHFFFAOYSA-N 0.000 description 1
- 239000012825 JNK inhibitor Substances 0.000 description 1
- 229940118135 JNK inhibitor Drugs 0.000 description 1
- VDYACOATPFOZIO-UBWHGVKJSA-N Kadsurenone Chemical compound C1=C(OC)C(OC)=CC=C1[C@@H]1[C@@H](C)[C@@]2(OC)C=C(CC=C)C(=O)C=C2O1 VDYACOATPFOZIO-UBWHGVKJSA-N 0.000 description 1
- 102000000079 Kainic Acid Receptors Human genes 0.000 description 1
- 108010069902 Kainic Acid Receptors Proteins 0.000 description 1
- 208000009319 Keratoconjunctivitis Sicca Diseases 0.000 description 1
- GGLZPLKKBSSKCX-YFKPBYRVSA-N L-ethionine Chemical compound CCSCC[C@H](N)C(O)=O GGLZPLKKBSSKCX-YFKPBYRVSA-N 0.000 description 1
- SFSJZXMDTNDWIX-YFKPBYRVSA-N L-homomethionine Chemical compound CSCCC[C@H](N)C(O)=O SFSJZXMDTNDWIX-YFKPBYRVSA-N 0.000 description 1
- FFEARJCKVFRZRR-BYPYZUCNSA-N L-methionine Chemical compound CSCC[C@H](N)C(O)=O FFEARJCKVFRZRR-BYPYZUCNSA-N 0.000 description 1
- 239000002067 L01XE06 - Dasatinib Substances 0.000 description 1
- 239000002136 L01XE07 - Lapatinib Substances 0.000 description 1
- 239000005536 L01XE08 - Nilotinib Substances 0.000 description 1
- JGPJQFOROWSRRS-UHFFFAOYSA-N LSM-2613 Chemical compound S1C=2N3C(C)=NN=C3CN=C(C=3C(=CC=CC=3)Cl)C=2C=C1CCC(=O)N1CCOCC1 JGPJQFOROWSRRS-UHFFFAOYSA-N 0.000 description 1
- 206010023642 Lacrimation decreased Diseases 0.000 description 1
- XNRVGTHNYCNCFF-UHFFFAOYSA-N Lapatinib ditosylate monohydrate Chemical compound O.CC1=CC=C(S(O)(=O)=O)C=C1.CC1=CC=C(S(O)(=O)=O)C=C1.O1C(CNCCS(=O)(=O)C)=CC=C1C1=CC=C(N=CN=C2NC=3C=C(Cl)C(OCC=4C=C(F)C=CC=4)=CC=3)C2=C1 XNRVGTHNYCNCFF-UHFFFAOYSA-N 0.000 description 1
- 208000009481 Laryngeal Edema Diseases 0.000 description 1
- 206010023845 Laryngeal oedema Diseases 0.000 description 1
- 206010024229 Leprosy Diseases 0.000 description 1
- 206010024264 Lethargy Diseases 0.000 description 1
- 240000007472 Leucaena leucocephala Species 0.000 description 1
- 235000010643 Leucaena leucocephala Nutrition 0.000 description 1
- 206010024641 Listeriosis Diseases 0.000 description 1
- GQYIWUVLTXOXAJ-UHFFFAOYSA-N Lomustine Chemical compound ClCCN(N=O)C(=O)NC1CCCCC1 GQYIWUVLTXOXAJ-UHFFFAOYSA-N 0.000 description 1
- 208000016604 Lyme disease Diseases 0.000 description 1
- 206010025323 Lymphomas Diseases 0.000 description 1
- 208000024556 Mendelian disease Diseases 0.000 description 1
- XOGTZOOQQBDUSI-UHFFFAOYSA-M Mesna Chemical compound [Na+].[O-]S(=O)(=O)CCS XOGTZOOQQBDUSI-UHFFFAOYSA-M 0.000 description 1
- 206010049567 Miller Fisher syndrome Diseases 0.000 description 1
- 229930192392 Mitomycin Natural products 0.000 description 1
- 229920000881 Modified starch Polymers 0.000 description 1
- 206010028034 Mouth ulceration Diseases 0.000 description 1
- 241000699666 Mus <mouse, genus> Species 0.000 description 1
- 101000591390 Mus musculus Neurotensin receptor type 2 Proteins 0.000 description 1
- 229940121948 Muscarinic receptor antagonist Drugs 0.000 description 1
- 208000007101 Muscle Cramp Diseases 0.000 description 1
- 208000000112 Myalgia Diseases 0.000 description 1
- 241000204031 Mycoplasma Species 0.000 description 1
- NWIBSHFKIJFRCO-WUDYKRTCSA-N Mytomycin Chemical compound C1N2C(C(C(C)=C(N)C3=O)=O)=C3[C@@H](COC(N)=O)[C@@]2(OC)[C@@H]2[C@H]1N2 NWIBSHFKIJFRCO-WUDYKRTCSA-N 0.000 description 1
- SECXISVLQFMRJM-UHFFFAOYSA-N N-Methylpyrrolidone Chemical compound CN1CCCC1=O SECXISVLQFMRJM-UHFFFAOYSA-N 0.000 description 1
- ZDZOTLJHXYCWBA-VCVYQWHSSA-N N-debenzoyl-N-(tert-butoxycarbonyl)-10-deacetyltaxol Chemical compound O([C@H]1[C@H]2[C@@](C([C@H](O)C3=C(C)[C@@H](OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=4C=CC=CC=4)C[C@]1(O)C3(C)C)=O)(C)[C@@H](O)C[C@H]1OC[C@]12OC(=O)C)C(=O)C1=CC=CC=C1 ZDZOTLJHXYCWBA-VCVYQWHSSA-N 0.000 description 1
- 206010028851 Necrosis Diseases 0.000 description 1
- 206010029155 Nephropathy toxic Diseases 0.000 description 1
- 208000009905 Neurofibromatoses Diseases 0.000 description 1
- 108010040718 Neurokinin-1 Receptors Proteins 0.000 description 1
- 244000061176 Nicotiana tabacum Species 0.000 description 1
- 235000002637 Nicotiana tabacum Nutrition 0.000 description 1
- 241001134446 Niveas Species 0.000 description 1
- 241000187654 Nocardia Species 0.000 description 1
- PHVGLTMQBUFIQQ-UHFFFAOYSA-N Nortryptiline Chemical compound C1CC2=CC=CC=C2C(=CCCNC)C2=CC=CC=C21 PHVGLTMQBUFIQQ-UHFFFAOYSA-N 0.000 description 1
- 108091093105 Nuclear DNA Proteins 0.000 description 1
- 206010030113 Oedema Diseases 0.000 description 1
- 206010030124 Oedema peripheral Diseases 0.000 description 1
- 206010030216 Oesophagitis Diseases 0.000 description 1
- 108700020796 Oncogene Proteins 0.000 description 1
- 208000007117 Oral Ulcer Diseases 0.000 description 1
- 206010067352 Osteoradionecrosis Diseases 0.000 description 1
- 229930012538 Paclitaxel Natural products 0.000 description 1
- 206010033546 Pallor Diseases 0.000 description 1
- 206010033557 Palpitations Diseases 0.000 description 1
- 206010033645 Pancreatitis Diseases 0.000 description 1
- 208000007542 Paresis Diseases 0.000 description 1
- AHOUBRCZNHFOSL-UHFFFAOYSA-N Paroxetine hydrochloride Natural products C1=CC(F)=CC=C1C1C(COC=2C=C3OCOC3=CC=2)CNCC1 AHOUBRCZNHFOSL-UHFFFAOYSA-N 0.000 description 1
- 208000000450 Pelvic Pain Diseases 0.000 description 1
- JGSARLDLIJGVTE-MBNYWOFBSA-N Penicillin G Chemical compound N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)CC1=CC=CC=C1 JGSARLDLIJGVTE-MBNYWOFBSA-N 0.000 description 1
- 239000004185 Penicillin G procaine Substances 0.000 description 1
- 108010087702 Penicillinase Proteins 0.000 description 1
- 102000035195 Peptidases Human genes 0.000 description 1
- 108091005804 Peptidases Proteins 0.000 description 1
- 208000005228 Pericardial Effusion Diseases 0.000 description 1
- 208000037581 Persistent Infection Diseases 0.000 description 1
- 206010034829 Pharyngeal oedema Diseases 0.000 description 1
- 102000015439 Phospholipases Human genes 0.000 description 1
- 108010064785 Phospholipases Proteins 0.000 description 1
- 102000045595 Phosphoprotein Phosphatases Human genes 0.000 description 1
- 108700019535 Phosphoprotein Phosphatases Proteins 0.000 description 1
- 229920003072 Plasdone™ povidone Polymers 0.000 description 1
- 208000005384 Pneumocystis Pneumonia Diseases 0.000 description 1
- 206010073755 Pneumocystis jirovecii pneumonia Diseases 0.000 description 1
- 206010035669 Pneumonia aspiration Diseases 0.000 description 1
- 206010035742 Pneumonitis Diseases 0.000 description 1
- 108010093965 Polymyxin B Proteins 0.000 description 1
- 108010040201 Polymyxins Proteins 0.000 description 1
- 229920001214 Polysorbate 60 Polymers 0.000 description 1
- 206010036410 Postoperative wound infection Diseases 0.000 description 1
- 206010036653 Presyncope Diseases 0.000 description 1
- 239000004365 Protease Substances 0.000 description 1
- 229940079156 Proteasome inhibitor Drugs 0.000 description 1
- 108010029485 Protein Isoforms Proteins 0.000 description 1
- 102000001708 Protein Isoforms Human genes 0.000 description 1
- 201000004681 Psoriasis Diseases 0.000 description 1
- 201000001263 Psoriatic Arthritis Diseases 0.000 description 1
- 208000036824 Psoriatic arthropathy Diseases 0.000 description 1
- 208000007123 Pulmonary Atelectasis Diseases 0.000 description 1
- 208000010378 Pulmonary Embolism Diseases 0.000 description 1
- 206010037423 Pulmonary oedema Diseases 0.000 description 1
- 206010037596 Pyelonephritis Diseases 0.000 description 1
- 208000009341 RNA Virus Infections Diseases 0.000 description 1
- 206010037855 Rash erythematous Diseases 0.000 description 1
- 241000700159 Rattus Species 0.000 description 1
- QEHOIJJIZXRMAN-UHFFFAOYSA-N Rebeccamycin Natural products OC1C(O)C(OC)C(CO)OC1N1C2=C3NC4=C(Cl)C=CC=C4C3=C3C(=O)NC(=O)C3=C2C2=CC=CC(Cl)=C21 QEHOIJJIZXRMAN-UHFFFAOYSA-N 0.000 description 1
- 108010008281 Recombinant Fusion Proteins Proteins 0.000 description 1
- 102000007056 Recombinant Fusion Proteins Human genes 0.000 description 1
- 208000005587 Refsum Disease Diseases 0.000 description 1
- 208000009921 Rheumatoid Nodule Diseases 0.000 description 1
- 208000011170 Semicircular Canal Dehiscence Diseases 0.000 description 1
- 208000036366 Sensation of pressure Diseases 0.000 description 1
- 206010040070 Septic Shock Diseases 0.000 description 1
- VYPSYNLAJGMNEJ-UHFFFAOYSA-N Silicium dioxide Chemical compound O=[Si]=O VYPSYNLAJGMNEJ-UHFFFAOYSA-N 0.000 description 1
- 108010003723 Single-Domain Antibodies Proteins 0.000 description 1
- 102220506570 Small ubiquitin-related modifier 2_K11R_mutation Human genes 0.000 description 1
- 206010062255 Soft tissue infection Diseases 0.000 description 1
- 229920002125 Sokalan® Polymers 0.000 description 1
- 208000005392 Spasm Diseases 0.000 description 1
- 206010041648 Splenic infarction Diseases 0.000 description 1
- 206010041660 Splenomegaly Diseases 0.000 description 1
- 241000193996 Streptococcus pyogenes Species 0.000 description 1
- 241000187747 Streptomyces Species 0.000 description 1
- ZSJLQEPLLKMAKR-UHFFFAOYSA-N Streptozotocin Natural products O=NN(C)C(=O)NC1C(O)OC(CO)C(O)C1O ZSJLQEPLLKMAKR-UHFFFAOYSA-N 0.000 description 1
- 208000002667 Subdural Hematoma Diseases 0.000 description 1
- 102100037346 Substance-P receptor Human genes 0.000 description 1
- OUUQCZGPVNCOIJ-UHFFFAOYSA-M Superoxide Chemical compound [O-][O] OUUQCZGPVNCOIJ-UHFFFAOYSA-M 0.000 description 1
- 208000031650 Surgical Wound Infection Diseases 0.000 description 1
- 208000001871 Tachycardia Diseases 0.000 description 1
- LGGHDPFKSSRQNS-UHFFFAOYSA-N Tariquidar Chemical compound C1=CC=CC2=CC(C(=O)NC3=CC(OC)=C(OC)C=C3C(=O)NC3=CC=C(C=C3)CCN3CCC=4C=C(C(=CC=4C3)OC)OC)=CN=C21 LGGHDPFKSSRQNS-UHFFFAOYSA-N 0.000 description 1
- WBWWGRHZICKQGZ-UHFFFAOYSA-N Taurocholic acid Natural products OC1CC2CC(O)CCC2(C)C2C1C1CCC(C(CCC(=O)NCCS(O)(=O)=O)C)C1(C)C(O)C2 WBWWGRHZICKQGZ-UHFFFAOYSA-N 0.000 description 1
- 229940123237 Taxane Drugs 0.000 description 1
- 206010043275 Teratogenicity Diseases 0.000 description 1
- 239000004098 Tetracycline Substances 0.000 description 1
- 229920002359 Tetronic® Polymers 0.000 description 1
- FOCVUCIESVLUNU-UHFFFAOYSA-N Thiotepa Chemical compound C1CN1P(N1CC1)(=S)N1CC1 FOCVUCIESVLUNU-UHFFFAOYSA-N 0.000 description 1
- 208000024799 Thyroid disease Diseases 0.000 description 1
- AUYYCJSJGJYCDS-LBPRGKRZSA-N Thyrolar Chemical compound IC1=CC(C[C@H](N)C(O)=O)=CC(I)=C1OC1=CC=C(O)C(I)=C1 AUYYCJSJGJYCDS-LBPRGKRZSA-N 0.000 description 1
- IVTVGDXNLFLDRM-HNNXBMFYSA-N Tomudex Chemical compound C=1C=C2NC(C)=NC(=O)C2=CC=1CN(C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)S1 IVTVGDXNLFLDRM-HNNXBMFYSA-N 0.000 description 1
- 229920001615 Tragacanth Polymers 0.000 description 1
- 102000011117 Transforming Growth Factor beta2 Human genes 0.000 description 1
- 101800000304 Transforming growth factor beta-2 Proteins 0.000 description 1
- 206010044565 Tremor Diseases 0.000 description 1
- 241000589884 Treponema pallidum Species 0.000 description 1
- 229940123445 Tricyclic antidepressant Drugs 0.000 description 1
- GSEJCLTVZPLZKY-UHFFFAOYSA-N Triethanolamine Chemical compound OCCN(CCO)CCO GSEJCLTVZPLZKY-UHFFFAOYSA-N 0.000 description 1
- 101710187830 Tumor necrosis factor receptor superfamily member 1B Proteins 0.000 description 1
- 102100033733 Tumor necrosis factor receptor superfamily member 1B Human genes 0.000 description 1
- 206010067584 Type 1 diabetes mellitus Diseases 0.000 description 1
- 208000025865 Ulcer Diseases 0.000 description 1
- 206010046306 Upper respiratory tract infection Diseases 0.000 description 1
- 208000024780 Urticaria Diseases 0.000 description 1
- HDOVUKNUBWVHOX-QMMMGPOBSA-N Valacyclovir Chemical compound N1C(N)=NC(=O)C2=C1N(COCCOC(=O)[C@@H](N)C(C)C)C=N2 HDOVUKNUBWVHOX-QMMMGPOBSA-N 0.000 description 1
- 206010070995 Vascular compression Diseases 0.000 description 1
- JXLYSJRDGCGARV-WWYNWVTFSA-N Vinblastine Natural products O=C(O[C@H]1[C@](O)(C(=O)OC)[C@@H]2N(C)c3c(cc(c(OC)c3)[C@]3(C(=O)OC)c4[nH]c5c(c4CCN4C[C@](O)(CC)C[C@H](C3)C4)cccc5)[C@@]32[C@H]2[C@@]1(CC)C=CCN2CC3)C JXLYSJRDGCGARV-WWYNWVTFSA-N 0.000 description 1
- 108020005202 Viral DNA Proteins 0.000 description 1
- FKAWLXNLHHIHLA-YCBIHMBMSA-N [(2r,3r,5r,7r,8s,9s)-2-[(1s,3s,4s,5r,6r,7e,9e,11e,13z)-14-cyano-3,5-dihydroxy-1-methoxy-4,6,8,9,13-pentamethyltetradeca-7,9,11,13-tetraenyl]-9-[(e)-3-[2-[(2s)-4-[[(2s,3s,4s)-4-(dimethylamino)-2,3-dihydroxy-5-methoxypentanoyl]amino]butan-2-yl]-1,3-oxazol-4 Chemical compound O1C([C@@H](C)CCNC(=O)[C@@H](O)[C@@H](O)[C@H](COC)N(C)C)=NC(\C=C\C[C@H]2[C@H]([C@H](O)C[C@]3(O2)C([C@@H](OP(O)(O)=O)[C@@H]([C@H](C[C@H](O)[C@H](C)[C@H](O)[C@H](C)\C=C(/C)\C(\C)=C\C=C\C(\C)=C/C#N)OC)O3)(C)C)C)=C1 FKAWLXNLHHIHLA-YCBIHMBMSA-N 0.000 description 1
- ATBOMIWRCZXYSZ-XZBBILGWSA-N [1-[2,3-dihydroxypropoxy(hydroxy)phosphoryl]oxy-3-hexadecanoyloxypropan-2-yl] (9e,12e)-octadeca-9,12-dienoate Chemical compound CCCCCCCCCCCCCCCC(=O)OCC(COP(O)(=O)OCC(O)CO)OC(=O)CCCCCCC\C=C\C\C=C\CCCCC ATBOMIWRCZXYSZ-XZBBILGWSA-N 0.000 description 1
- WPVFJKSGQUFQAP-UHFFFAOYSA-N [2-[(2-amino-6-oxo-3h-purin-9-yl)methoxy]-3-hydroxypropyl] 2-amino-3-methylbutanoate Chemical compound N1C(N)=NC(=O)C2=C1N(COC(CO)COC(=O)C(N)C(C)C)C=N2 WPVFJKSGQUFQAP-UHFFFAOYSA-N 0.000 description 1
- LCZMCBVUOCAXCX-UHFFFAOYSA-N ac1l3gr2 Chemical compound O=C1OC2CC(C(C)(C)C)C34C(O)C(=O)OC4OC41C32CC1OC(=O)C(C)C41O.O1C2(C(=O)O3)C4(O)C(C)C(=O)OC4C(O)C42C3CC(C(C)(C)C)C42C1OC(=O)C2O.O1C2(C(=O)O3)C4(O)C(C)C(=O)OC4C(O)C42C3CC(C(C)(C)C)C42C1OC(=O)C2O LCZMCBVUOCAXCX-UHFFFAOYSA-N 0.000 description 1
- 235000010489 acacia gum Nutrition 0.000 description 1
- 230000001133 acceleration Effects 0.000 description 1
- VJHCJDRQFCCTHL-UHFFFAOYSA-N acetic acid 2,3,4,5,6-pentahydroxyhexanal Chemical compound CC(O)=O.OCC(O)C(O)C(O)C(O)C=O VJHCJDRQFCCTHL-UHFFFAOYSA-N 0.000 description 1
- ZUAAPNNKRHMPKG-UHFFFAOYSA-N acetic acid;butanedioic acid;methanol;propane-1,2-diol Chemical compound OC.CC(O)=O.CC(O)CO.OC(=O)CCC(O)=O ZUAAPNNKRHMPKG-UHFFFAOYSA-N 0.000 description 1
- SPTSIOTYTJZTOG-UHFFFAOYSA-N acetic acid;octadecanoic acid Chemical compound CC(O)=O.CCCCCCCCCCCCCCCCCC(O)=O SPTSIOTYTJZTOG-UHFFFAOYSA-N 0.000 description 1
- 102000034337 acetylcholine receptors Human genes 0.000 description 1
- 239000002253 acid Substances 0.000 description 1
- 150000007513 acids Chemical class 0.000 description 1
- 229940125665 acridine carboxamide Drugs 0.000 description 1
- 230000003044 adaptive effect Effects 0.000 description 1
- 230000033289 adaptive immune response Effects 0.000 description 1
- 239000000853 adhesive Substances 0.000 description 1
- 230000001070 adhesive effect Effects 0.000 description 1
- 229940009456 adriamycin Drugs 0.000 description 1
- 208000030597 adult Refsum disease Diseases 0.000 description 1
- 229920000615 alginic acid Polymers 0.000 description 1
- 235000010443 alginic acid Nutrition 0.000 description 1
- 150000005215 alkyl ethers Chemical class 0.000 description 1
- SHGAZHPCJJPHSC-YCNIQYBTSA-N all-trans-retinoic acid Chemical compound OC(=O)\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C SHGAZHPCJJPHSC-YCNIQYBTSA-N 0.000 description 1
- 229940125528 allosteric inhibitor Drugs 0.000 description 1
- 235000012741 allura red AC Nutrition 0.000 description 1
- 239000004191 allura red AC Substances 0.000 description 1
- AWUCVROLDVIAJX-UHFFFAOYSA-N alpha-glycerophosphate Natural products OCC(O)COP(O)(O)=O AWUCVROLDVIAJX-UHFFFAOYSA-N 0.000 description 1
- VREFGVBLTWBCJP-UHFFFAOYSA-N alprazolam Chemical compound C12=CC(Cl)=CC=C2N2C(C)=NN=C2CN=C1C1=CC=CC=C1 VREFGVBLTWBCJP-UHFFFAOYSA-N 0.000 description 1
- SNAAJJQQZSMGQD-UHFFFAOYSA-N aluminum magnesium Chemical compound [Mg].[Al] SNAAJJQQZSMGQD-UHFFFAOYSA-N 0.000 description 1
- JKOQGQFVAUAYPM-UHFFFAOYSA-N amifostine Chemical compound NCCCNCCSP(O)(O)=O JKOQGQFVAUAYPM-UHFFFAOYSA-N 0.000 description 1
- 229960001097 amifostine Drugs 0.000 description 1
- 229960003896 aminopterin Drugs 0.000 description 1
- 230000003321 amplification Effects 0.000 description 1
- 229960001220 amsacrine Drugs 0.000 description 1
- XCPGHVQEEXUHNC-UHFFFAOYSA-N amsacrine Chemical compound COC1=CC(NS(C)(=O)=O)=CC=C1NC1=C(C=CC=C2)C2=NC2=CC=CC=C12 XCPGHVQEEXUHNC-UHFFFAOYSA-N 0.000 description 1
- 238000004458 analytical method Methods 0.000 description 1
- 230000036783 anaphylactic response Effects 0.000 description 1
- 208000003455 anaphylaxis Diseases 0.000 description 1
- 210000003484 anatomy Anatomy 0.000 description 1
- 208000007502 anemia Diseases 0.000 description 1
- 229940045799 anthracyclines and related substance Drugs 0.000 description 1
- 230000002424 anti-apoptotic effect Effects 0.000 description 1
- 230000001078 anti-cholinergic effect Effects 0.000 description 1
- 230000003474 anti-emetic effect Effects 0.000 description 1
- 230000000843 anti-fungal effect Effects 0.000 description 1
- 230000000340 anti-metabolite Effects 0.000 description 1
- 230000000118 anti-neoplastic effect Effects 0.000 description 1
- 230000000890 antigenic effect Effects 0.000 description 1
- 229940100197 antimetabolite Drugs 0.000 description 1
- 239000002256 antimetabolite Substances 0.000 description 1
- 239000000164 antipsychotic agent Substances 0.000 description 1
- 229940071731 antivert Drugs 0.000 description 1
- 239000003920 antivertigo agent Substances 0.000 description 1
- 229950001852 apafant Drugs 0.000 description 1
- 238000013459 approach Methods 0.000 description 1
- 230000009118 appropriate response Effects 0.000 description 1
- 210000005097 arteria cerebelosa anteroinferior Anatomy 0.000 description 1
- 210000001367 artery Anatomy 0.000 description 1
- 206010003246 arthritis Diseases 0.000 description 1
- 235000010323 ascorbic acid Nutrition 0.000 description 1
- 239000011668 ascorbic acid Substances 0.000 description 1
- 229960005070 ascorbic acid Drugs 0.000 description 1
- 201000009807 aspiration pneumonia Diseases 0.000 description 1
- 125000004429 atom Chemical group 0.000 description 1
- 201000008937 atopic dermatitis Diseases 0.000 description 1
- 210000003926 auditory cortex Anatomy 0.000 description 1
- 208000037979 autoimmune inflammatory disease Diseases 0.000 description 1
- 230000005784 autoimmunity Effects 0.000 description 1
- 210000003050 axon Anatomy 0.000 description 1
- 229960002170 azathioprine Drugs 0.000 description 1
- LMEKQMALGUDUQG-UHFFFAOYSA-N azathioprine Chemical compound CN1C=NC([N+]([O-])=O)=C1SC1=NC=NC2=C1NC=N2 LMEKQMALGUDUQG-UHFFFAOYSA-N 0.000 description 1
- 229960000794 baclofen Drugs 0.000 description 1
- 229910052788 barium Inorganic materials 0.000 description 1
- DSAJWYNOEDNPEQ-UHFFFAOYSA-N barium atom Chemical compound [Ba] DSAJWYNOEDNPEQ-UHFFFAOYSA-N 0.000 description 1
- 239000002585 base Substances 0.000 description 1
- 210000002469 basement membrane Anatomy 0.000 description 1
- 210000001841 basilar artery Anatomy 0.000 description 1
- 229960004669 basiliximab Drugs 0.000 description 1
- 229960002707 bendamustine Drugs 0.000 description 1
- YTKUWDBFDASYHO-UHFFFAOYSA-N bendamustine Chemical compound ClCCN(CCCl)C1=CC=C2N(C)C(CCCC(O)=O)=NC2=C1 YTKUWDBFDASYHO-UHFFFAOYSA-N 0.000 description 1
- 229960000686 benzalkonium chloride Drugs 0.000 description 1
- 229960004217 benzyl alcohol Drugs 0.000 description 1
- CADWTSSKOVRVJC-UHFFFAOYSA-N benzyl(dimethyl)azanium;chloride Chemical compound [Cl-].C[NH+](C)CC1=CC=CC=C1 CADWTSSKOVRVJC-UHFFFAOYSA-N 0.000 description 1
- 229940118531 bicillin Drugs 0.000 description 1
- 239000011230 binding agent Substances 0.000 description 1
- 230000008512 biological response Effects 0.000 description 1
- CGVWPQOFHSAKRR-NDEPHWFRSA-N biricodar Chemical compound COC1=C(OC)C(OC)=CC(C(=O)C(=O)N2[C@@H](CCCC2)C(=O)OC(CCCC=2C=NC=CC=2)CCCC=2C=NC=CC=2)=C1 CGVWPQOFHSAKRR-NDEPHWFRSA-N 0.000 description 1
- 229950005124 biricodar Drugs 0.000 description 1
- 229920001400 block copolymer Polymers 0.000 description 1
- 231100001015 blood dyscrasias Toxicity 0.000 description 1
- 230000036765 blood level Effects 0.000 description 1
- 230000036772 blood pressure Effects 0.000 description 1
- 230000036770 blood supply Effects 0.000 description 1
- 230000036760 body temperature Effects 0.000 description 1
- 230000008468 bone growth Effects 0.000 description 1
- 210000001185 bone marrow Anatomy 0.000 description 1
- 229940094219 bonine Drugs 0.000 description 1
- 210000005013 brain tissue Anatomy 0.000 description 1
- 229940077737 brain-derived neurotrophic factor Drugs 0.000 description 1
- 125000004799 bromophenyl group Chemical group 0.000 description 1
- 206010006451 bronchitis Diseases 0.000 description 1
- 229960005520 bryostatin Drugs 0.000 description 1
- MJQUEDHRCUIRLF-TVIXENOKSA-N bryostatin 1 Chemical compound C([C@@H]1CC(/[C@@H]([C@@](C(C)(C)/C=C/2)(O)O1)OC(=O)/C=C/C=C/CCC)=C\C(=O)OC)[C@H]([C@@H](C)O)OC(=O)C[C@H](O)C[C@@H](O1)C[C@H](OC(C)=O)C(C)(C)[C@]1(O)C[C@@H]1C\C(=C\C(=O)OC)C[C@H]\2O1 MJQUEDHRCUIRLF-TVIXENOKSA-N 0.000 description 1
- MUIWQCKLQMOUAT-AKUNNTHJSA-N bryostatin 20 Natural products COC(=O)C=C1C[C@@]2(C)C[C@]3(O)O[C@](C)(C[C@@H](O)CC(=O)O[C@](C)(C[C@@]4(C)O[C@](O)(CC5=CC(=O)O[C@]45C)C(C)(C)C=C[C@@](C)(C1)O2)[C@@H](C)O)C[C@H](OC(=O)C(C)(C)C)C3(C)C MUIWQCKLQMOUAT-AKUNNTHJSA-N 0.000 description 1
- 229960002092 busulfan Drugs 0.000 description 1
- VJEONQKOZGKCAK-UHFFFAOYSA-N caffeine Natural products CN1C(=O)N(C)C(=O)C2=C1C=CN2C VJEONQKOZGKCAK-UHFFFAOYSA-N 0.000 description 1
- 229960001948 caffeine Drugs 0.000 description 1
- 229910052791 calcium Inorganic materials 0.000 description 1
- 229960005069 calcium Drugs 0.000 description 1
- 235000008207 calcium folinate Nutrition 0.000 description 1
- 239000011687 calcium folinate Substances 0.000 description 1
- UHHRFSOMMCWGSO-UHFFFAOYSA-L calcium glycerophosphate Chemical compound [Ca+2].OCC(CO)OP([O-])([O-])=O UHHRFSOMMCWGSO-UHFFFAOYSA-L 0.000 description 1
- 229940095618 calcium glycerophosphate Drugs 0.000 description 1
- 235000019299 calcium glycerylphosphate Nutrition 0.000 description 1
- MKJXYGKVIBWPFZ-UHFFFAOYSA-L calcium lactate Chemical compound [Ca+2].CC(O)C([O-])=O.CC(O)C([O-])=O MKJXYGKVIBWPFZ-UHFFFAOYSA-L 0.000 description 1
- 239000001527 calcium lactate Substances 0.000 description 1
- 229960002401 calcium lactate Drugs 0.000 description 1
- 235000011086 calcium lactate Nutrition 0.000 description 1
- 239000001506 calcium phosphate Substances 0.000 description 1
- 229930182747 calyculin Natural products 0.000 description 1
- VSJKWCGYPAHWDS-FQEVSTJZSA-N camptothecin Chemical compound C1=CC=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 VSJKWCGYPAHWDS-FQEVSTJZSA-N 0.000 description 1
- 229940127093 camptothecin Drugs 0.000 description 1
- 229940095731 candida albicans Drugs 0.000 description 1
- 229960004117 capecitabine Drugs 0.000 description 1
- 229960004602 capreomycin Drugs 0.000 description 1
- 229960002504 capsaicin Drugs 0.000 description 1
- 235000017663 capsaicin Nutrition 0.000 description 1
- 229960000623 carbamazepine Drugs 0.000 description 1
- 239000004202 carbamide Substances 0.000 description 1
- 150000001720 carbohydrates Chemical class 0.000 description 1
- 235000014633 carbohydrates Nutrition 0.000 description 1
- 229920003123 carboxymethyl cellulose sodium Polymers 0.000 description 1
- 229940063834 carboxymethylcellulose sodium Drugs 0.000 description 1
- 230000002612 cardiopulmonary effect Effects 0.000 description 1
- 231100000259 cardiotoxicity Toxicity 0.000 description 1
- 210000000269 carotid artery external Anatomy 0.000 description 1
- 235000010418 carrageenan Nutrition 0.000 description 1
- 229920001525 carrageenan Polymers 0.000 description 1
- 239000000679 carrageenan Substances 0.000 description 1
- 229940113118 carrageenan Drugs 0.000 description 1
- 239000004359 castor oil Substances 0.000 description 1
- 235000019438 castor oil Nutrition 0.000 description 1
- 230000003197 catalytic effect Effects 0.000 description 1
- 230000001364 causal effect Effects 0.000 description 1
- 229960002129 cefixime Drugs 0.000 description 1
- OKBVVJOGVLARMR-QSWIMTSFSA-N cefixime Chemical compound S1C(N)=NC(C(=N\OCC(O)=O)\C(=O)N[C@@H]2C(N3C(=C(C=C)CS[C@@H]32)C(O)=O)=O)=C1 OKBVVJOGVLARMR-QSWIMTSFSA-N 0.000 description 1
- 229960001668 cefuroxime Drugs 0.000 description 1
- JFPVXVDWJQMJEE-IZRZKJBUSA-N cefuroxime Chemical compound N([C@@H]1C(N2C(=C(COC(N)=O)CS[C@@H]21)C(O)=O)=O)C(=O)\C(=N/OC)C1=CC=CO1 JFPVXVDWJQMJEE-IZRZKJBUSA-N 0.000 description 1
- 230000010261 cell growth Effects 0.000 description 1
- 230000009087 cell motility Effects 0.000 description 1
- 230000006800 cellular catabolic process Effects 0.000 description 1
- 230000001413 cellular effect Effects 0.000 description 1
- 208000005675 central hearing loss Diseases 0.000 description 1
- 208000015114 central nervous system disease Diseases 0.000 description 1
- 210000001638 cerebellum Anatomy 0.000 description 1
- 230000002490 cerebral effect Effects 0.000 description 1
- 206010008118 cerebral infarction Diseases 0.000 description 1
- 239000002738 chelating agent Substances 0.000 description 1
- OIQPTROHQCGFEF-UHFFFAOYSA-L chembl1371409 Chemical compound [Na+].[Na+].OC1=CC=C2C=C(S([O-])(=O)=O)C=CC2=C1N=NC1=CC=C(S([O-])(=O)=O)C=C1 OIQPTROHQCGFEF-UHFFFAOYSA-L 0.000 description 1
- CEZCCHQBSQPRMU-UHFFFAOYSA-L chembl174821 Chemical compound [Na+].[Na+].COC1=CC(S([O-])(=O)=O)=C(C)C=C1N=NC1=C(O)C=CC2=CC(S([O-])(=O)=O)=CC=C12 CEZCCHQBSQPRMU-UHFFFAOYSA-L 0.000 description 1
- CDSBFDCCJJDFCV-CKZSCMLPSA-N chembl2107777 Chemical compound C([C@H]1CC[C@@]2(C(=O)N(C3=CC=C(C=C32)OCC)S(=O)(=O)C=2C(=CC(=CC=2)C(=O)NC(C)(C)C)OC)CC1)CN1CCOCC1 CDSBFDCCJJDFCV-CKZSCMLPSA-N 0.000 description 1
- IHOVFYSQUDPMCN-DBEBIPAYSA-N chembl444172 Chemical compound C([C@H](COC=1C2=CC=CN=C2C=CC=1)O)N(CC1)CCN1[C@@H]1C2=CC=CC=C2[C@H]2C(F)(F)[C@H]2C2=CC=CC=C12 IHOVFYSQUDPMCN-DBEBIPAYSA-N 0.000 description 1
- JCKYGMPEJWAADB-UHFFFAOYSA-N chlorambucil Chemical compound OC(=O)CCCC1=CC=C(N(CCCl)CCCl)C=C1 JCKYGMPEJWAADB-UHFFFAOYSA-N 0.000 description 1
- 229960004630 chlorambucil Drugs 0.000 description 1
- 201000001352 cholecystitis Diseases 0.000 description 1
- 150000001840 cholesterol esters Chemical class 0.000 description 1
- 230000002759 chromosomal effect Effects 0.000 description 1
- 201000005795 chronic inflammatory demyelinating polyneuritis Diseases 0.000 description 1
- DERZBLKQOCDDDZ-JLHYYAGUSA-N cinnarizine Chemical compound C1CN(C(C=2C=CC=CC=2)C=2C=CC=CC=2)CCN1C\C=C\C1=CC=CC=C1 DERZBLKQOCDDDZ-JLHYYAGUSA-N 0.000 description 1
- 229960000876 cinnarizine Drugs 0.000 description 1
- 229960003405 ciprofloxacin Drugs 0.000 description 1
- 229960002436 cladribine Drugs 0.000 description 1
- WDDPHFBMKLOVOX-AYQXTPAHSA-N clofarabine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1F WDDPHFBMKLOVOX-AYQXTPAHSA-N 0.000 description 1
- 229960000928 clofarabine Drugs 0.000 description 1
- 229960004022 clotrimazole Drugs 0.000 description 1
- VNFPBHJOKIVQEB-UHFFFAOYSA-N clotrimazole Chemical compound ClC1=CC=CC=C1C(N1C=NC=C1)(C=1C=CC=CC=1)C1=CC=CC=C1 VNFPBHJOKIVQEB-UHFFFAOYSA-N 0.000 description 1
- 238000011260 co-administration Methods 0.000 description 1
- 229940047766 co-trimoxazole Drugs 0.000 description 1
- 210000003952 cochlear nucleus Anatomy 0.000 description 1
- 208000010877 cognitive disease Diseases 0.000 description 1
- 229940075614 colloidal silicon dioxide Drugs 0.000 description 1
- 229940088505 compazine Drugs 0.000 description 1
- 230000000295 complement effect Effects 0.000 description 1
- 230000001010 compromised effect Effects 0.000 description 1
- 230000002153 concerted effect Effects 0.000 description 1
- 230000001143 conditioned effect Effects 0.000 description 1
- 208000034494 congenital cholesteatoma Diseases 0.000 description 1
- 201000005890 congenital diaphragmatic hernia Diseases 0.000 description 1
- 201000006901 congenital syphilis Diseases 0.000 description 1
- JGBBVDFNZSRLIF-UHFFFAOYSA-N conivaptan Chemical compound C12=CC=CC=C2C=2[N]C(C)=NC=2CCN1C(=O)C(C=C1)=CC=C1NC(=O)C1=CC=CC=C1C1=CC=CC=C1 JGBBVDFNZSRLIF-UHFFFAOYSA-N 0.000 description 1
- 229960000562 conivaptan Drugs 0.000 description 1
- 210000002808 connective tissue Anatomy 0.000 description 1
- 230000008602 contraction Effects 0.000 description 1
- 208000029078 coronary artery disease Diseases 0.000 description 1
- 238000012937 correction Methods 0.000 description 1
- 201000008107 cortical deafness Diseases 0.000 description 1
- ALEXXDVDDISNDU-JZYPGELDSA-N cortisol 21-acetate Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)COC(=O)C)(O)[C@@]1(C)C[C@@H]2O ALEXXDVDDISNDU-JZYPGELDSA-N 0.000 description 1
- OTGAHJPFNKQGAE-UHFFFAOYSA-N cresatin Chemical compound CC(=O)OC1=CC=CC(C)=C1 OTGAHJPFNKQGAE-UHFFFAOYSA-N 0.000 description 1
- 229960000862 cresatin Drugs 0.000 description 1
- 239000013078 crystal Substances 0.000 description 1
- 208000007085 cutaneous syphilis Diseases 0.000 description 1
- 229940097362 cyclodextrins Drugs 0.000 description 1
- 208000031513 cyst Diseases 0.000 description 1
- 229960000684 cytarabine Drugs 0.000 description 1
- 210000000805 cytoplasm Anatomy 0.000 description 1
- 210000004292 cytoskeleton Anatomy 0.000 description 1
- 230000001086 cytosolic effect Effects 0.000 description 1
- 239000000824 cytostatic agent Substances 0.000 description 1
- 230000001085 cytostatic effect Effects 0.000 description 1
- 230000003013 cytotoxicity Effects 0.000 description 1
- 231100000135 cytotoxicity Toxicity 0.000 description 1
- GVJHHUAWPYXKBD-UHFFFAOYSA-N d-alpha-tocopherol Natural products OC1=C(C)C(C)=C2OC(CCCC(C)CCCC(C)CCCC(C)C)(C)CCC2=C1C GVJHHUAWPYXKBD-UHFFFAOYSA-N 0.000 description 1
- 229960003901 dacarbazine Drugs 0.000 description 1
- 229960002806 daclizumab Drugs 0.000 description 1
- 208000019000 darkening of skin Diseases 0.000 description 1
- 229960002448 dasatinib Drugs 0.000 description 1
- 230000034994 death Effects 0.000 description 1
- 229960003603 decitabine Drugs 0.000 description 1
- 230000002950 deficient Effects 0.000 description 1
- 230000006735 deficit Effects 0.000 description 1
- 230000003111 delayed effect Effects 0.000 description 1
- 230000002939 deleterious effect Effects 0.000 description 1
- SIBFMRAHSCSBRP-UHFFFAOYSA-N denudatin B Natural products COC1=C2OC(C(C)C2(OC)C=C(CC=C)C1=O)c3ccc(OC)c(OC)c3 SIBFMRAHSCSBRP-UHFFFAOYSA-N 0.000 description 1
- 230000030609 dephosphorylation Effects 0.000 description 1
- 238000006209 dephosphorylation reaction Methods 0.000 description 1
- 230000000779 depleting effect Effects 0.000 description 1
- 230000003831 deregulation Effects 0.000 description 1
- 230000001627 detrimental effect Effects 0.000 description 1
- 229960000605 dexrazoxane Drugs 0.000 description 1
- 229960005215 dichloroacetic acid Drugs 0.000 description 1
- XXJWXESWEXIICW-UHFFFAOYSA-N diethylene glycol monoethyl ether Chemical compound CCOCCOCCO XXJWXESWEXIICW-UHFFFAOYSA-N 0.000 description 1
- NLORYLAYLIXTID-ISLYRVAYSA-N diethylstilbestrol diphosphate Chemical compound C=1C=C(OP(O)(O)=O)C=CC=1C(/CC)=C(\CC)C1=CC=C(OP(O)(O)=O)C=C1 NLORYLAYLIXTID-ISLYRVAYSA-N 0.000 description 1
- 238000007865 diluting Methods 0.000 description 1
- FSBVERYRVPGNGG-UHFFFAOYSA-N dimagnesium dioxido-bis[[oxido(oxo)silyl]oxy]silane hydrate Chemical compound O.[Mg+2].[Mg+2].[O-][Si](=O)O[Si]([O-])([O-])O[Si]([O-])=O FSBVERYRVPGNGG-UHFFFAOYSA-N 0.000 description 1
- 239000000539 dimer Substances 0.000 description 1
- 230000003292 diminished effect Effects 0.000 description 1
- 229960003724 dimyristoylphosphatidylcholine Drugs 0.000 description 1
- 229910001882 dioxygen Inorganic materials 0.000 description 1
- 229960000520 diphenhydramine Drugs 0.000 description 1
- ZPWVASYFFYYZEW-UHFFFAOYSA-L dipotassium hydrogen phosphate Chemical compound [K+].[K+].OP([O-])([O-])=O ZPWVASYFFYYZEW-UHFFFAOYSA-L 0.000 description 1
- 235000019797 dipotassium phosphate Nutrition 0.000 description 1
- 229910000396 dipotassium phosphate Inorganic materials 0.000 description 1
- 230000006806 disease prevention Effects 0.000 description 1
- IVKWXPBUMQZFCW-UHFFFAOYSA-L disodium;2-(2,4,5,7-tetraiodo-3-oxido-6-oxoxanthen-9-yl)benzoate;hydrate Chemical compound O.[Na+].[Na+].[O-]C(=O)C1=CC=CC=C1C1=C2C=C(I)C(=O)C(I)=C2OC2=C(I)C([O-])=C(I)C=C21 IVKWXPBUMQZFCW-UHFFFAOYSA-L 0.000 description 1
- 238000006073 displacement reaction Methods 0.000 description 1
- 208000007784 diverticulitis Diseases 0.000 description 1
- VSJKWCGYPAHWDS-UHFFFAOYSA-N dl-camptothecin Natural products C1=CC=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)C5(O)CC)C4=NC2=C1 VSJKWCGYPAHWDS-UHFFFAOYSA-N 0.000 description 1
- 229960003668 docetaxel Drugs 0.000 description 1
- 231100000371 dose-limiting toxicity Toxicity 0.000 description 1
- 231100000673 dose–response relationship Toxicity 0.000 description 1
- 229960004679 doxorubicin Drugs 0.000 description 1
- 229940099182 dramamine Drugs 0.000 description 1
- 229940075060 driminate Drugs 0.000 description 1
- 239000006196 drop Substances 0.000 description 1
- 239000003937 drug carrier Substances 0.000 description 1
- 238000007876 drug discovery Methods 0.000 description 1
- 201000006549 dyspepsia Diseases 0.000 description 1
- 208000031083 ear cancer Diseases 0.000 description 1
- 229950010033 ebselen Drugs 0.000 description 1
- 230000002500 effect on skin Effects 0.000 description 1
- 239000003995 emulsifying agent Substances 0.000 description 1
- 239000000839 emulsion Substances 0.000 description 1
- 230000002124 endocrine Effects 0.000 description 1
- 206010014801 endophthalmitis Diseases 0.000 description 1
- 210000002889 endothelial cell Anatomy 0.000 description 1
- 229930013356 epothilone Natural products 0.000 description 1
- 150000003883 epothilone derivatives Chemical class 0.000 description 1
- 229960003649 eribulin Drugs 0.000 description 1
- UFNVPOGXISZXJD-XJPMSQCNSA-N eribulin Chemical compound C([C@H]1CC[C@@H]2O[C@@H]3[C@H]4O[C@H]5C[C@](O[C@H]4[C@H]2O1)(O[C@@H]53)CC[C@@H]1O[C@H](C(C1)=C)CC1)C(=O)C[C@@H]2[C@@H](OC)[C@@H](C[C@H](O)CN)O[C@H]2C[C@@H]2C(=C)[C@H](C)C[C@H]1O2 UFNVPOGXISZXJD-XJPMSQCNSA-N 0.000 description 1
- HCZKYJDFEPMADG-UHFFFAOYSA-N erythro-nordihydroguaiaretic acid Natural products C=1C=C(O)C(O)=CC=1CC(C)C(C)CC1=CC=C(O)C(O)=C1 HCZKYJDFEPMADG-UHFFFAOYSA-N 0.000 description 1
- 235000012732 erythrosine Nutrition 0.000 description 1
- 239000004174 erythrosine Substances 0.000 description 1
- 208000006881 esophagitis Diseases 0.000 description 1
- FRPJXPJMRWBBIH-RBRWEJTLSA-N estramustine Chemical compound ClCCN(CCCl)C(=O)OC1=CC=C2[C@H]3CC[C@](C)([C@H](CC4)O)[C@@H]4[C@@H]3CCC2=C1 FRPJXPJMRWBBIH-RBRWEJTLSA-N 0.000 description 1
- 229960001842 estramustine Drugs 0.000 description 1
- 108020004067 estrogen-related receptors Proteins 0.000 description 1
- 229960003199 etacrynic acid Drugs 0.000 description 1
- LVGKNOAMLMIIKO-QXMHVHEDSA-N ethyl oleate Chemical compound CCCCCCCC\C=C/CCCCCCCC(=O)OCC LVGKNOAMLMIIKO-QXMHVHEDSA-N 0.000 description 1
- 229940093471 ethyl oleate Drugs 0.000 description 1
- 229960005420 etoposide Drugs 0.000 description 1
- VJJPUSNTGOMMGY-MRVIYFEKSA-N etoposide Chemical compound COC1=C(O)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@@H](O[C@H]3[C@@H]([C@@H](O)[C@@H]4O[C@H](C)OC[C@H]4O3)O)[C@@H]3[C@@H]2C(OC3)=O)=C1 VJJPUSNTGOMMGY-MRVIYFEKSA-N 0.000 description 1
- ZVYVPGLRVWUPMP-FYSMJZIKSA-N exatecan Chemical compound C1C[C@H](N)C2=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC3=CC(F)=C(C)C1=C32 ZVYVPGLRVWUPMP-FYSMJZIKSA-N 0.000 description 1
- 229950009429 exatecan Drugs 0.000 description 1
- 229950000484 exisulind Drugs 0.000 description 1
- 230000004424 eye movement Effects 0.000 description 1
- 208000011318 facial edema Diseases 0.000 description 1
- 230000001815 facial effect Effects 0.000 description 1
- 210000001097 facial muscle Anatomy 0.000 description 1
- 229960004396 famciclovir Drugs 0.000 description 1
- GGXKWVWZWMLJEH-UHFFFAOYSA-N famcyclovir Chemical compound N1=C(N)N=C2N(CCC(COC(=O)C)COC(C)=O)C=NC2=C1 GGXKWVWZWMLJEH-UHFFFAOYSA-N 0.000 description 1
- 235000019240 fast green FCF Nutrition 0.000 description 1
- 210000000630 fibrocyte Anatomy 0.000 description 1
- 239000000945 filler Substances 0.000 description 1
- 238000010304 firing Methods 0.000 description 1
- 230000003890 fistula Effects 0.000 description 1
- 150000002212 flavone derivatives Chemical class 0.000 description 1
- 238000007667 floating Methods 0.000 description 1
- 229960000390 fludarabine Drugs 0.000 description 1
- GIUYCYHIANZCFB-FJFJXFQQSA-N fludarabine phosphate Chemical compound C1=NC=2C(N)=NC(F)=NC=2N1[C@@H]1O[C@H](COP(O)(O)=O)[C@@H](O)[C@@H]1O GIUYCYHIANZCFB-FJFJXFQQSA-N 0.000 description 1
- MHMNJMPURVTYEJ-UHFFFAOYSA-N fluorescein-5-isothiocyanate Chemical compound O1C(=O)C2=CC(N=C=S)=CC=C2C21C1=CC=C(O)C=C1OC1=CC(O)=CC=C21 MHMNJMPURVTYEJ-UHFFFAOYSA-N 0.000 description 1
- 229940124307 fluoroquinolone Drugs 0.000 description 1
- 229960002949 fluorouracil Drugs 0.000 description 1
- 235000008191 folinic acid Nutrition 0.000 description 1
- 239000011672 folinic acid Substances 0.000 description 1
- 235000013305 food Nutrition 0.000 description 1
- 229960000297 fosfestrol Drugs 0.000 description 1
- ZZUFCTLCJUWOSV-UHFFFAOYSA-N furosemide Chemical compound C1=C(Cl)C(S(=O)(=O)N)=CC(C(O)=O)=C1NCC1=CC=CO1 ZZUFCTLCJUWOSV-UHFFFAOYSA-N 0.000 description 1
- 229960003883 furosemide Drugs 0.000 description 1
- 230000004927 fusion Effects 0.000 description 1
- UIWYJDYFSGRHKR-UHFFFAOYSA-N gadolinium atom Chemical compound [Gd] UIWYJDYFSGRHKR-UHFFFAOYSA-N 0.000 description 1
- 229960002963 ganciclovir Drugs 0.000 description 1
- 210000000609 ganglia Anatomy 0.000 description 1
- 230000002496 gastric effect Effects 0.000 description 1
- 239000008273 gelatin Substances 0.000 description 1
- 229920000159 gelatin Polymers 0.000 description 1
- 229940014259 gelatin Drugs 0.000 description 1
- 235000019322 gelatine Nutrition 0.000 description 1
- 235000011852 gelatine desserts Nutrition 0.000 description 1
- SDUQYLNIPVEERB-QPPQHZFASA-N gemcitabine Chemical compound O=C1N=C(N)C=CN1[C@H]1C(F)(F)[C@H](O)[C@@H](CO)O1 SDUQYLNIPVEERB-QPPQHZFASA-N 0.000 description 1
- 229960005277 gemcitabine Drugs 0.000 description 1
- 102000034356 gene-regulatory proteins Human genes 0.000 description 1
- 108091006104 gene-regulatory proteins Proteins 0.000 description 1
- 230000002068 genetic effect Effects 0.000 description 1
- SQOJOAFXDQDRGF-MMQTXUMRSA-N ginkgolide-b Chemical compound O[C@H]([C@]12[C@H](C(C)(C)C)C[C@H]3OC4=O)C(=O)O[C@H]2O[C@]24[C@@]13[C@@H](O)[C@@H]1OC(=O)[C@@H](C)[C@]21O SQOJOAFXDQDRGF-MMQTXUMRSA-N 0.000 description 1
- 229930182494 ginsenoside Natural products 0.000 description 1
- 239000011521 glass Substances 0.000 description 1
- 235000011187 glycerol Nutrition 0.000 description 1
- ZEMPKEQAKRGZGQ-XOQCFJPHSA-N glycerol triricinoleate Natural products CCCCCC[C@@H](O)CC=CCCCCCCCC(=O)OC[C@@H](COC(=O)CCCCCCCC=CC[C@@H](O)CCCCCC)OC(=O)CCCCCCCC=CC[C@H](O)CCCCCC ZEMPKEQAKRGZGQ-XOQCFJPHSA-N 0.000 description 1
- 229940075507 glyceryl monostearate Drugs 0.000 description 1
- 239000003102 growth factor Substances 0.000 description 1
- SCMLRESZJCKCTC-KMYQRJGFSA-N gtpl8173 Chemical compound C12=CC=C(CSCC)C=C2C2=C(CNC3=O)C3=C3C4=CC(CSCC)=CC=C4N4C3=C2N1[C@]1(C)[C@@](O)(C(=O)OC)C[C@H]4O1 SCMLRESZJCKCTC-KMYQRJGFSA-N 0.000 description 1
- 235000010417 guar gum Nutrition 0.000 description 1
- 239000000665 guar gum Substances 0.000 description 1
- 229960002154 guar gum Drugs 0.000 description 1
- 230000037308 hair color Effects 0.000 description 1
- 230000036541 health Effects 0.000 description 1
- 230000003862 health status Effects 0.000 description 1
- 208000014951 hematologic disease Diseases 0.000 description 1
- 230000002489 hematologic effect Effects 0.000 description 1
- 208000018706 hematopoietic system disease Diseases 0.000 description 1
- 208000006750 hematuria Diseases 0.000 description 1
- 206010019465 hemiparesis Diseases 0.000 description 1
- 201000002802 hemorrhagic cystitis Diseases 0.000 description 1
- 230000002440 hepatic effect Effects 0.000 description 1
- 208000006454 hepatitis Diseases 0.000 description 1
- 231100000283 hepatitis Toxicity 0.000 description 1
- 230000007686 hepatotoxicity Effects 0.000 description 1
- 239000000833 heterodimer Substances 0.000 description 1
- 238000012766 histopathologic analysis Methods 0.000 description 1
- SFSJZXMDTNDWIX-UHFFFAOYSA-N homomethionine Natural products CSCCCC(N)C(O)=O SFSJZXMDTNDWIX-UHFFFAOYSA-N 0.000 description 1
- 230000003054 hormonal effect Effects 0.000 description 1
- 229940048921 humira Drugs 0.000 description 1
- 229920001477 hydrophilic polymer Polymers 0.000 description 1
- 235000019447 hydroxyethyl cellulose Nutrition 0.000 description 1
- 239000001863 hydroxypropyl cellulose Substances 0.000 description 1
- 229940031704 hydroxypropyl methylcellulose phthalate Drugs 0.000 description 1
- 229920003132 hydroxypropyl methylcellulose phthalate Polymers 0.000 description 1
- 229940071676 hydroxypropylcellulose Drugs 0.000 description 1
- 230000009610 hypersensitivity Effects 0.000 description 1
- 201000009939 hypertensive encephalopathy Diseases 0.000 description 1
- 208000034783 hypoesthesia Diseases 0.000 description 1
- 229960000908 idarubicin Drugs 0.000 description 1
- HOMGKSMUEGBAAB-UHFFFAOYSA-N ifosfamide Chemical compound ClCCNP1(=O)OCCCN1CCCl HOMGKSMUEGBAAB-UHFFFAOYSA-N 0.000 description 1
- 229960001101 ifosfamide Drugs 0.000 description 1
- 238000003384 imaging method Methods 0.000 description 1
- 229960002751 imiquimod Drugs 0.000 description 1
- DOUYETYNHWVLEO-UHFFFAOYSA-N imiquimod Chemical compound C1=CC=CC2=C3N(CC(C)C)C=NC3=C(N)N=C21 DOUYETYNHWVLEO-UHFFFAOYSA-N 0.000 description 1
- 208000026278 immune system disease Diseases 0.000 description 1
- 229940121354 immunomodulator Drugs 0.000 description 1
- 230000002584 immunomodulator Effects 0.000 description 1
- 230000007365 immunoregulation Effects 0.000 description 1
- 238000002513 implantation Methods 0.000 description 1
- 238000000338 in vitro Methods 0.000 description 1
- 229960004657 indocyanine green Drugs 0.000 description 1
- MOFVSTNWEDAEEK-UHFFFAOYSA-M indocyanine green Chemical compound [Na+].[O-]S(=O)(=O)CCCCN1C2=CC=C3C=CC=CC3=C2C(C)(C)C1=CC=CC=CC=CC1=[N+](CCCCS([O-])(=O)=O)C2=CC=C(C=CC=C3)C3=C2C1(C)C MOFVSTNWEDAEEK-UHFFFAOYSA-M 0.000 description 1
- 230000001939 inductive effect Effects 0.000 description 1
- 210000004969 inflammatory cell Anatomy 0.000 description 1
- 210000000067 inner hair cell Anatomy 0.000 description 1
- 230000030214 innervation Effects 0.000 description 1
- 238000003780 insertion Methods 0.000 description 1
- 230000037431 insertion Effects 0.000 description 1
- 230000002452 interceptive effect Effects 0.000 description 1
- 238000010253 intravenous injection Methods 0.000 description 1
- UWKQSNNFCGGAFS-XIFFEERXSA-N irinotecan Chemical compound C1=C2C(CC)=C3CN(C(C4=C([C@@](C(=O)OC4)(O)CC)C=4)=O)C=4C3=NC2=CC=C1OC(=O)N(CC1)CCC1N1CCCCC1 UWKQSNNFCGGAFS-XIFFEERXSA-N 0.000 description 1
- 229960004768 irinotecan Drugs 0.000 description 1
- 229950005254 irofulven Drugs 0.000 description 1
- NICJCIQSJJKZAH-AWEZNQCLSA-N irofulven Chemical compound O=C([C@@]1(O)C)C2=CC(C)=C(CO)C2=C(C)C21CC2 NICJCIQSJJKZAH-AWEZNQCLSA-N 0.000 description 1
- 229910052742 iron Inorganic materials 0.000 description 1
- 230000000622 irritating effect Effects 0.000 description 1
- 229940074320 iso-sulfan blue Drugs 0.000 description 1
- 238000002955 isolation Methods 0.000 description 1
- 229960004130 itraconazole Drugs 0.000 description 1
- FABUFPQFXZVHFB-CFWQTKTJSA-N ixabepilone Chemical compound C/C([C@@H]1C[C@@H]2O[C@]2(C)CCC[C@@H]([C@@H]([C@H](C)C(=O)C(C)(C)[C@H](O)CC(=O)N1)O)C)=C\C1=CSC(C)=N1 FABUFPQFXZVHFB-CFWQTKTJSA-N 0.000 description 1
- 229960002014 ixabepilone Drugs 0.000 description 1
- 210000001847 jaw Anatomy 0.000 description 1
- 230000003907 kidney function Effects 0.000 description 1
- 210000002664 langerhans' cell Anatomy 0.000 description 1
- 229950010652 laniquidar Drugs 0.000 description 1
- TULGGJGJQXESOO-UHFFFAOYSA-N laniquidar Chemical compound C12=CC=CC=C2CCN2C(C(=O)OC)=CN=C2C1=C1CCN(CCC=2C=CC(OCC=3N=C4C=CC=CC4=CC=3)=CC=2)CC1 TULGGJGJQXESOO-UHFFFAOYSA-N 0.000 description 1
- 229960004891 lapatinib Drugs 0.000 description 1
- GGXICVAJURFBLW-CEYXHVGTSA-N latanoprost Chemical compound CC(C)OC(=O)CCC\C=C/C[C@H]1[C@@H](O)C[C@@H](O)[C@@H]1CC[C@@H](O)CCC1=CC=CC=C1 GGXICVAJURFBLW-CEYXHVGTSA-N 0.000 description 1
- 235000010445 lecithin Nutrition 0.000 description 1
- 239000000787 lecithin Substances 0.000 description 1
- GOTYRUGSSMKFNF-UHFFFAOYSA-N lenalidomide Chemical compound C1C=2C(N)=CC=CC=2C(=O)N1C1CCC(=O)NC1=O GOTYRUGSSMKFNF-UHFFFAOYSA-N 0.000 description 1
- 230000003902 lesion Effects 0.000 description 1
- 229960001691 leucovorin Drugs 0.000 description 1
- 229960002293 leucovorin calcium Drugs 0.000 description 1
- 239000003446 ligand Substances 0.000 description 1
- 239000012669 liquid formulation Substances 0.000 description 1
- 230000007056 liver toxicity Effects 0.000 description 1
- PPHTXRNHTVLQED-UHFFFAOYSA-N lixivaptan Chemical compound CC1=CC=C(F)C=C1C(=O)NC(C=C1Cl)=CC=C1C(=O)N1C2=CC=CC=C2CN2C=CC=C2C1 PPHTXRNHTVLQED-UHFFFAOYSA-N 0.000 description 1
- 229960002247 lomustine Drugs 0.000 description 1
- 235000014659 low sodium diet Nutrition 0.000 description 1
- 239000000314 lubricant Substances 0.000 description 1
- 210000002751 lymph Anatomy 0.000 description 1
- 210000004698 lymphocyte Anatomy 0.000 description 1
- 229940041033 macrolides Drugs 0.000 description 1
- 229950000547 mafosfamide Drugs 0.000 description 1
- 239000000391 magnesium silicate Substances 0.000 description 1
- 235000019792 magnesium silicate Nutrition 0.000 description 1
- 229910052919 magnesium silicate Inorganic materials 0.000 description 1
- 208000011736 mal de Debarquement Diseases 0.000 description 1
- 230000036210 malignancy Effects 0.000 description 1
- 208000022924 malignant ear neoplasm Diseases 0.000 description 1
- 229950002736 marizomib Drugs 0.000 description 1
- 229960003951 masoprocol Drugs 0.000 description 1
- HCZKYJDFEPMADG-TXEJJXNPSA-N masoprocol Chemical compound C([C@H](C)[C@H](C)CC=1C=C(O)C(O)=CC=1)C1=CC=C(O)C(O)=C1 HCZKYJDFEPMADG-TXEJJXNPSA-N 0.000 description 1
- 230000007246 mechanism Effects 0.000 description 1
- 210000000412 mechanoreceptor Anatomy 0.000 description 1
- 108091008704 mechanoreceptors Proteins 0.000 description 1
- HAWPXGHAZFHHAD-UHFFFAOYSA-N mechlorethamine Chemical compound ClCCN(C)CCCl HAWPXGHAZFHHAD-UHFFFAOYSA-N 0.000 description 1
- 229960004961 mechlorethamine Drugs 0.000 description 1
- 238000013160 medical therapy Methods 0.000 description 1
- SGDBTWWWUNNDEQ-LBPRGKRZSA-N melphalan Chemical compound OC(=O)[C@@H](N)CC1=CC=C(N(CCCl)CCCl)C=C1 SGDBTWWWUNNDEQ-LBPRGKRZSA-N 0.000 description 1
- 229960001924 melphalan Drugs 0.000 description 1
- 210000003071 memory t lymphocyte Anatomy 0.000 description 1
- 230000006609 metabolic stress Effects 0.000 description 1
- 229930182817 methionine Natural products 0.000 description 1
- 229960004452 methionine Drugs 0.000 description 1
- 125000002496 methyl group Chemical group [H]C([H])([H])* 0.000 description 1
- CXKWCBBOMKCUKX-UHFFFAOYSA-M methylene blue Chemical compound [Cl-].C1=CC(N(C)C)=CC2=[S+]C3=CC(N(C)C)=CC=C3N=C21 CXKWCBBOMKCUKX-UHFFFAOYSA-M 0.000 description 1
- 229960000907 methylthioninium chloride Drugs 0.000 description 1
- 238000002406 microsurgery Methods 0.000 description 1
- 230000005012 migration Effects 0.000 description 1
- 238000013508 migration Methods 0.000 description 1
- CFCUWKMKBJTWLW-BKHRDMLASA-N mithramycin Chemical compound O([C@@H]1C[C@@H](O[C@H](C)[C@H]1O)OC=1C=C2C=C3C[C@H]([C@@H](C(=O)C3=C(O)C2=C(O)C=1C)O[C@@H]1O[C@H](C)[C@@H](O)[C@H](O[C@@H]2O[C@H](C)[C@H](O)[C@H](O[C@@H]3O[C@H](C)[C@@H](O)[C@@](C)(O)C3)C2)C1)[C@H](OC)C(=O)[C@@H](O)[C@@H](C)O)[C@H]1C[C@@H](O)[C@H](O)[C@@H](C)O1 CFCUWKMKBJTWLW-BKHRDMLASA-N 0.000 description 1
- 229960004857 mitomycin Drugs 0.000 description 1
- 229960000350 mitotane Drugs 0.000 description 1
- 229960001156 mitoxantrone Drugs 0.000 description 1
- KKZJGLLVHKMTCM-UHFFFAOYSA-N mitoxantrone Chemical compound O=C1C2=C(O)C=CC(O)=C2C(=O)C2=C1C(NCCNCCO)=CC=C2NCCNCCO KKZJGLLVHKMTCM-UHFFFAOYSA-N 0.000 description 1
- 238000002156 mixing Methods 0.000 description 1
- 239000001788 mono and diglycerides of fatty acids Substances 0.000 description 1
- 210000001616 monocyte Anatomy 0.000 description 1
- 150000004682 monohydrates Chemical class 0.000 description 1
- 201000003152 motion sickness Diseases 0.000 description 1
- 210000002161 motor neuron Anatomy 0.000 description 1
- 210000000214 mouth Anatomy 0.000 description 1
- 208000018962 mouth sore Diseases 0.000 description 1
- 229950000546 mozavaptan Drugs 0.000 description 1
- 239000003149 muscarinic antagonist Substances 0.000 description 1
- 230000002107 myocardial effect Effects 0.000 description 1
- 208000010125 myocardial infarction Diseases 0.000 description 1
- 208000031225 myocardial ischemia Diseases 0.000 description 1
- XBGNERSKEKDZDS-UHFFFAOYSA-N n-[2-(dimethylamino)ethyl]acridine-4-carboxamide Chemical compound C1=CC=C2N=C3C(C(=O)NCCN(C)C)=CC=CC3=CC2=C1 XBGNERSKEKDZDS-UHFFFAOYSA-N 0.000 description 1
- XJZRYHGTQLKUDO-UHFFFAOYSA-N n-[5-(6,11-dihydropyrrolo[2,1-c][1,4]benzodiazepine-5-carbonyl)pyridin-2-yl]-5-fluoro-2-methylbenzamide Chemical compound CC1=CC=C(F)C=C1C(=O)NC1=CC=C(C(=O)N2C3=CC=CC=C3CN3C=CC=C3C2)C=N1 XJZRYHGTQLKUDO-UHFFFAOYSA-N 0.000 description 1
- 229930014626 natural product Natural products 0.000 description 1
- 230000017074 necrotic cell death Effects 0.000 description 1
- IXOXBSCIXZEQEQ-UHTZMRCNSA-N nelarabine Chemical compound C1=NC=2C(OC)=NC(N)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1O IXOXBSCIXZEQEQ-UHTZMRCNSA-N 0.000 description 1
- 229960000801 nelarabine Drugs 0.000 description 1
- 230000007694 nephrotoxicity Effects 0.000 description 1
- 230000008035 nerve activity Effects 0.000 description 1
- 229960000808 netilmicin Drugs 0.000 description 1
- ZBGPYVZLYBDXKO-HILBYHGXSA-N netilmycin Chemical compound O([C@@H]1[C@@H](N)C[C@H]([C@@H]([C@H]1O)O[C@@H]1[C@]([C@H](NC)[C@@H](O)CO1)(C)O)NCC)[C@H]1OC(CN)=CC[C@H]1N ZBGPYVZLYBDXKO-HILBYHGXSA-N 0.000 description 1
- 210000000118 neural pathway Anatomy 0.000 description 1
- 230000010004 neural pathway Effects 0.000 description 1
- 201000004931 neurofibromatosis Diseases 0.000 description 1
- 208000029974 neurofibrosarcoma Diseases 0.000 description 1
- 230000000926 neurological effect Effects 0.000 description 1
- 208000008795 neuromyelitis optica Diseases 0.000 description 1
- 230000003955 neuronal function Effects 0.000 description 1
- 230000007514 neuronal growth Effects 0.000 description 1
- 239000003901 neurotransmitter uptake inhibitor Substances 0.000 description 1
- 230000011242 neutrophil chemotaxis Effects 0.000 description 1
- 229960002715 nicotine Drugs 0.000 description 1
- SNICXCGAKADSCV-UHFFFAOYSA-N nicotine Natural products CN1CCCC1C1=CC=CN=C1 SNICXCGAKADSCV-UHFFFAOYSA-N 0.000 description 1
- 229960001346 nilotinib Drugs 0.000 description 1
- HHZIURLSWUIHRB-UHFFFAOYSA-N nilotinib Chemical compound C1=NC(C)=CN1C1=CC(NC(=O)C=2C=C(NC=3N=C(C=CN=3)C=3C=NC=CC=3)C(C)=CC=2)=CC(C(F)(F)F)=C1 HHZIURLSWUIHRB-UHFFFAOYSA-N 0.000 description 1
- 231100000344 non-irritating Toxicity 0.000 description 1
- 229960001158 nortriptyline Drugs 0.000 description 1
- 238000003199 nucleic acid amplification method Methods 0.000 description 1
- 231100000862 numbness Toxicity 0.000 description 1
- 208000022035 objective vertigo Diseases 0.000 description 1
- 229960000435 oblimersen Drugs 0.000 description 1
- MIMNFCVQODTQDP-NDLVEFNKSA-N oblimersen Chemical compound O=C1NC(=O)C(C)=CN1[C@@H]1O[C@H](COP(S)(=O)O[C@@H]2[C@H](O[C@H](C2)N2C3=NC=NC(N)=C3N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=NC=NC(N)=C3N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)CO)[C@@H](O)C1 MIMNFCVQODTQDP-NDLVEFNKSA-N 0.000 description 1
- YYZUSRORWSJGET-UHFFFAOYSA-N octanoic acid ethyl ester Natural products CCCCCCCC(=O)OCC YYZUSRORWSJGET-UHFFFAOYSA-N 0.000 description 1
- 229920004914 octoxynol-40 Polymers 0.000 description 1
- 229960001699 ofloxacin Drugs 0.000 description 1
- 229940127249 oral antibiotic Drugs 0.000 description 1
- 229940100691 oral capsule Drugs 0.000 description 1
- 229940124624 oral corticosteroid Drugs 0.000 description 1
- 230000008520 organization Effects 0.000 description 1
- 230000011164 ossification Effects 0.000 description 1
- DWAFYCQODLXJNR-BNTLRKBRSA-L oxaliplatin Chemical compound O1C(=O)C(=O)O[Pt]11N[C@@H]2CCCC[C@H]2N1 DWAFYCQODLXJNR-BNTLRKBRSA-L 0.000 description 1
- 229960001756 oxaliplatin Drugs 0.000 description 1
- 229960001592 paclitaxel Drugs 0.000 description 1
- 244000045947 parasite Species 0.000 description 1
- 230000003071 parasitic effect Effects 0.000 description 1
- 229960002296 paroxetine Drugs 0.000 description 1
- 230000001314 paroxysmal effect Effects 0.000 description 1
- 208000008016 pathologic nystagmus Diseases 0.000 description 1
- 229960005079 pemetrexed Drugs 0.000 description 1
- QOFFJEBXNKRSPX-ZDUSSCGKSA-N pemetrexed Chemical compound C1=N[C]2NC(N)=NC(=O)C2=C1CCC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 QOFFJEBXNKRSPX-ZDUSSCGKSA-N 0.000 description 1
- 230000035515 penetration Effects 0.000 description 1
- 235000019370 penicillin G procaine Nutrition 0.000 description 1
- 229940056362 penicillin g procaine Drugs 0.000 description 1
- 229950009506 penicillinase Drugs 0.000 description 1
- 229960002340 pentostatin Drugs 0.000 description 1
- FPVKHBSQESCIEP-JQCXWYLXSA-N pentostatin Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(N=CNC[C@H]2O)=C2N=C1 FPVKHBSQESCIEP-JQCXWYLXSA-N 0.000 description 1
- 208000008494 pericarditis Diseases 0.000 description 1
- 210000001428 peripheral nervous system Anatomy 0.000 description 1
- 238000012831 peritoneal equilibrium test Methods 0.000 description 1
- 208000022821 personality disease Diseases 0.000 description 1
- 238000002823 phage display Methods 0.000 description 1
- 239000008024 pharmaceutical diluent Substances 0.000 description 1
- 229940124531 pharmaceutical excipient Drugs 0.000 description 1
- 230000000144 pharmacologic effect Effects 0.000 description 1
- 229950000688 phenothiazine Drugs 0.000 description 1
- VEIJXOFPJWWIIJ-DCXFOUBQSA-N phomactin Chemical compound C1C\C(C)=C\CC[C@@]2(C)O[C@@H]2C(=O)[C@@H]2CC[C@@H](C)[C@@]1(C)[C@H]2C=O VEIJXOFPJWWIIJ-DCXFOUBQSA-N 0.000 description 1
- 229930184946 phomactin Natural products 0.000 description 1
- 150000008105 phosphatidylcholines Chemical class 0.000 description 1
- 150000008104 phosphatidylethanolamines Chemical class 0.000 description 1
- 229940067605 phosphatidylethanolamines Drugs 0.000 description 1
- 150000003904 phospholipids Chemical class 0.000 description 1
- 230000004962 physiological condition Effects 0.000 description 1
- 230000035479 physiological effects, processes and functions Effects 0.000 description 1
- NJBFOOCLYDNZJN-UHFFFAOYSA-N pipobroman Chemical compound BrCCC(=O)N1CCN(C(=O)CCBr)CC1 NJBFOOCLYDNZJN-UHFFFAOYSA-N 0.000 description 1
- 229960000952 pipobroman Drugs 0.000 description 1
- PEZPMAYDXJQYRV-UHFFFAOYSA-N pixantrone Chemical compound O=C1C2=CN=CC=C2C(=O)C2=C1C(NCCN)=CC=C2NCCN PEZPMAYDXJQYRV-UHFFFAOYSA-N 0.000 description 1
- 229960004403 pixantrone Drugs 0.000 description 1
- 230000036470 plasma concentration Effects 0.000 description 1
- 239000004014 plasticizer Substances 0.000 description 1
- 229960003171 plicamycin Drugs 0.000 description 1
- 201000000317 pneumocystosis Diseases 0.000 description 1
- 229960000502 poloxamer Drugs 0.000 description 1
- 229940044476 poloxamer 407 Drugs 0.000 description 1
- 102000054765 polymorphisms of proteins Human genes 0.000 description 1
- 208000005987 polymyositis Diseases 0.000 description 1
- 229920000024 polymyxin B Polymers 0.000 description 1
- 229960005266 polymyxin b Drugs 0.000 description 1
- 229940041153 polymyxins Drugs 0.000 description 1
- 229940068965 polysorbates Drugs 0.000 description 1
- 229920006316 polyvinylpyrrolidine Polymers 0.000 description 1
- UVSMNLNDYGZFPF-UHFFFAOYSA-N pomalidomide Chemical compound O=C1C=2C(N)=CC=CC=2C(=O)N1C1CCC(=O)NC1=O UVSMNLNDYGZFPF-UHFFFAOYSA-N 0.000 description 1
- 229940126027 positive allosteric modulator Drugs 0.000 description 1
- 230000034190 positive regulation of NF-kappaB transcription factor activity Effects 0.000 description 1
- 238000012636 positron electron tomography Methods 0.000 description 1
- 238000012877 positron emission topography Methods 0.000 description 1
- 230000001242 postsynaptic effect Effects 0.000 description 1
- 230000001124 posttranscriptional effect Effects 0.000 description 1
- LWIHDJKSTIGBAC-UHFFFAOYSA-K potassium phosphate Substances [K+].[K+].[K+].[O-]P([O-])([O-])=O LWIHDJKSTIGBAC-UHFFFAOYSA-K 0.000 description 1
- 229940069328 povidone Drugs 0.000 description 1
- 230000002335 preservative effect Effects 0.000 description 1
- 238000003825 pressing Methods 0.000 description 1
- 210000005215 presynaptic neuron Anatomy 0.000 description 1
- 238000002203 pretreatment Methods 0.000 description 1
- 229960001807 prilocaine Drugs 0.000 description 1
- MVFGUOIZUNYYSO-UHFFFAOYSA-N prilocaine Chemical compound CCCNC(C)C(=O)NC1=CC=CC=C1C MVFGUOIZUNYYSO-UHFFFAOYSA-N 0.000 description 1
- 125000002924 primary amino group Chemical group [H]N([H])* 0.000 description 1
- DBABZHXKTCFAPX-UHFFFAOYSA-N probenecid Chemical compound CCCN(CCC)S(=O)(=O)C1=CC=C(C(O)=O)C=C1 DBABZHXKTCFAPX-UHFFFAOYSA-N 0.000 description 1
- 229960003081 probenecid Drugs 0.000 description 1
- CPTBDICYNRMXFX-UHFFFAOYSA-N procarbazine Chemical compound CNNCC1=CC=C(C(=O)NC(C)C)C=C1 CPTBDICYNRMXFX-UHFFFAOYSA-N 0.000 description 1
- 229960000624 procarbazine Drugs 0.000 description 1
- 206010036807 progressive multifocal leukoencephalopathy Diseases 0.000 description 1
- 230000002062 proliferating effect Effects 0.000 description 1
- 230000035755 proliferation Effects 0.000 description 1
- 239000003207 proteasome inhibitor Substances 0.000 description 1
- 230000002633 protecting effect Effects 0.000 description 1
- 230000001681 protective effect Effects 0.000 description 1
- 229940121649 protein inhibitor Drugs 0.000 description 1
- 239000012268 protein inhibitor Substances 0.000 description 1
- 229940112971 protopic Drugs 0.000 description 1
- 208000020016 psychiatric disease Diseases 0.000 description 1
- 208000005333 pulmonary edema Diseases 0.000 description 1
- 208000005069 pulmonary fibrosis Diseases 0.000 description 1
- 201000002948 purulent labyrinthitis Diseases 0.000 description 1
- ZLIBICFPKPWGIZ-UHFFFAOYSA-N pyrimethanil Chemical compound CC1=CC(C)=NC(NC=2C=CC=CC=2)=N1 ZLIBICFPKPWGIZ-UHFFFAOYSA-N 0.000 description 1
- 229960004432 raltitrexed Drugs 0.000 description 1
- ZAHRKKWIAAJSAO-UHFFFAOYSA-N rapamycin Natural products COCC(O)C(=C/C(C)C(=O)CC(OC(=O)C1CCCCN1C(=O)C(=O)C2(O)OC(CC(OC)C(=CC=CC=CC(C)CC(C)C(=O)C)C)CCC2C)C(C)CC3CCC(O)C(C3)OC)C ZAHRKKWIAAJSAO-UHFFFAOYSA-N 0.000 description 1
- 230000009103 reabsorption Effects 0.000 description 1
- 230000009257 reactivity Effects 0.000 description 1
- 229960005567 rebeccamycin Drugs 0.000 description 1
- INSACQSBHKIWNS-QZQSLCQPSA-N rebeccamycin Chemical compound O[C@@H]1[C@@H](O)[C@H](OC)[C@@H](CO)O[C@H]1N1C2=C3N=C4[C](Cl)C=CC=C4C3=C3C(=O)NC(=O)C3=C2C2=CC=CC(Cl)=C21 INSACQSBHKIWNS-QZQSLCQPSA-N 0.000 description 1
- 229940044551 receptor antagonist Drugs 0.000 description 1
- 239000002464 receptor antagonist Substances 0.000 description 1
- 210000003370 receptor cell Anatomy 0.000 description 1
- 108091006082 receptor inhibitors Proteins 0.000 description 1
- 238000011084 recovery Methods 0.000 description 1
- 230000007115 recruitment Effects 0.000 description 1
- 238000004064 recycling Methods 0.000 description 1
- 230000008929 regeneration Effects 0.000 description 1
- 238000011069 regeneration method Methods 0.000 description 1
- 230000009711 regulatory function Effects 0.000 description 1
- 229940116176 remicade Drugs 0.000 description 1
- 230000002336 repolarization Effects 0.000 description 1
- 208000023504 respiratory system disease Diseases 0.000 description 1
- 229940053174 restasis Drugs 0.000 description 1
- 230000000284 resting effect Effects 0.000 description 1
- 230000000717 retained effect Effects 0.000 description 1
- 229940120975 revlimid Drugs 0.000 description 1
- 229940061969 rheumatrex Drugs 0.000 description 1
- 206010039083 rhinitis Diseases 0.000 description 1
- PYWVYCXTNDRMGF-UHFFFAOYSA-N rhodamine B Chemical compound [Cl-].C=12C=CC(=[N+](CC)CC)C=C2OC2=CC(N(CC)CC)=CC=C2C=1C1=CC=CC=C1C(O)=O PYWVYCXTNDRMGF-UHFFFAOYSA-N 0.000 description 1
- 201000005404 rubella Diseases 0.000 description 1
- VHXNKPBCCMUMSW-FQEVSTJZSA-N rubitecan Chemical compound C1=CC([N+]([O-])=O)=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 VHXNKPBCCMUMSW-FQEVSTJZSA-N 0.000 description 1
- 229950009213 rubitecan Drugs 0.000 description 1
- 210000005077 saccule Anatomy 0.000 description 1
- NGWSFRIPKNWYAO-SHTIJGAHSA-N salinosporamide A Chemical compound C([C@@H]1[C@H](O)[C@]23C(=O)O[C@]2([C@H](C(=O)N3)CCCl)C)CCC=C1 NGWSFRIPKNWYAO-SHTIJGAHSA-N 0.000 description 1
- NGWSFRIPKNWYAO-UHFFFAOYSA-N salinosporamide A Natural products N1C(=O)C(CCCl)C2(C)OC(=O)C21C(O)C1CCCC=C1 NGWSFRIPKNWYAO-UHFFFAOYSA-N 0.000 description 1
- 210000004116 schwann cell Anatomy 0.000 description 1
- 230000009291 secondary effect Effects 0.000 description 1
- 230000003248 secreting effect Effects 0.000 description 1
- 230000036421 sense of balance Effects 0.000 description 1
- 210000001044 sensory neuron Anatomy 0.000 description 1
- 230000020341 sensory perception of pain Effects 0.000 description 1
- 201000001223 septic arthritis Diseases 0.000 description 1
- 230000036303 septic shock Effects 0.000 description 1
- 238000009589 serological test Methods 0.000 description 1
- 239000003772 serotonin uptake inhibitor Substances 0.000 description 1
- 201000003850 serous labyrinthitis Diseases 0.000 description 1
- 229960002073 sertraline Drugs 0.000 description 1
- VGKDLMBJGBXTGI-SJCJKPOMSA-N sertraline Chemical compound C1([C@@H]2CC[C@@H](C3=CC=CC=C32)NC)=CC=C(Cl)C(Cl)=C1 VGKDLMBJGBXTGI-SJCJKPOMSA-N 0.000 description 1
- 210000002966 serum Anatomy 0.000 description 1
- 208000037851 severe atopic dermatitis Diseases 0.000 description 1
- 238000004904 shortening Methods 0.000 description 1
- 230000019491 signal transduction Effects 0.000 description 1
- 229960002930 sirolimus Drugs 0.000 description 1
- BTGNGJJLZOIYID-UHFFFAOYSA-N sivelestat Chemical compound C1=CC(OC(=O)C(C)(C)C)=CC=C1S(=O)(=O)NC1=CC=CC=C1C(=O)NCC(O)=O BTGNGJJLZOIYID-UHFFFAOYSA-N 0.000 description 1
- 229950009343 sivelestat Drugs 0.000 description 1
- 231100000046 skin rash Toxicity 0.000 description 1
- 230000000391 smoking effect Effects 0.000 description 1
- 235000010378 sodium ascorbate Nutrition 0.000 description 1
- PPASLZSBLFJQEF-RKJRWTFHSA-M sodium ascorbate Substances [Na+].OC[C@@H](O)[C@H]1OC(=O)C(O)=C1[O-] PPASLZSBLFJQEF-RKJRWTFHSA-M 0.000 description 1
- 229960005055 sodium ascorbate Drugs 0.000 description 1
- 239000003195 sodium channel blocking agent Substances 0.000 description 1
- 239000011780 sodium chloride Substances 0.000 description 1
- APSBXTVYXVQYAB-UHFFFAOYSA-M sodium docusate Chemical compound [Na+].CCCCC(CC)COC(=O)CC(S([O-])(=O)=O)C(=O)OCC(CC)CCCC APSBXTVYXVQYAB-UHFFFAOYSA-M 0.000 description 1
- 159000000000 sodium salts Chemical class 0.000 description 1
- 229940080352 sodium stearoyl lactylate Drugs 0.000 description 1
- PPASLZSBLFJQEF-RXSVEWSESA-M sodium-L-ascorbate Chemical compound [Na+].OC[C@H](O)[C@H]1OC(=O)C(O)=C1[O-] PPASLZSBLFJQEF-RXSVEWSESA-M 0.000 description 1
- NLUFDZBOHMOBOE-UHFFFAOYSA-M sodium;2-[[4-(diethylamino)phenyl]-(4-diethylazaniumylidenecyclohexa-2,5-dien-1-ylidene)methyl]benzene-1,4-disulfonate Chemical compound [Na+].C1=CC(N(CC)CC)=CC=C1C(C=1C(=CC=C(C=1)S([O-])(=O)=O)S([O-])(=O)=O)=C1C=CC(=[N+](CC)CC)C=C1 NLUFDZBOHMOBOE-UHFFFAOYSA-M 0.000 description 1
- JJICLMJFIKGAAU-UHFFFAOYSA-M sodium;2-amino-9-(1,3-dihydroxypropan-2-yloxymethyl)purin-6-olate Chemical compound [Na+].NC1=NC([O-])=C2N=CN(COC(CO)CO)C2=N1 JJICLMJFIKGAAU-UHFFFAOYSA-M 0.000 description 1
- KVMUSGMZFRRCAS-UHFFFAOYSA-N sodium;5-oxo-1-(4-sulfophenyl)-4-[(4-sulfophenyl)diazenyl]-4h-pyrazole-3-carboxylic acid Chemical compound [Na+].OC(=O)C1=NN(C=2C=CC(=CC=2)S(O)(=O)=O)C(=O)C1N=NC1=CC=C(S(O)(=O)=O)C=C1 KVMUSGMZFRRCAS-UHFFFAOYSA-N 0.000 description 1
- 230000000392 somatic effect Effects 0.000 description 1
- 239000008347 soybean phospholipid Substances 0.000 description 1
- 208000005198 spinal stenosis Diseases 0.000 description 1
- 238000009987 spinning Methods 0.000 description 1
- 210000002205 spiral ligament of cochlea Anatomy 0.000 description 1
- 230000002269 spontaneous effect Effects 0.000 description 1
- 230000000087 stabilizing effect Effects 0.000 description 1
- 239000008174 sterile solution Substances 0.000 description 1
- 229960001052 streptozocin Drugs 0.000 description 1
- ZSJLQEPLLKMAKR-GKHCUFPYSA-N streptozocin Chemical compound O=NN(C)C(=O)N[C@H]1[C@@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O ZSJLQEPLLKMAKR-GKHCUFPYSA-N 0.000 description 1
- 210000002386 strial marginal cell Anatomy 0.000 description 1
- 208000022037 subjective vertigo Diseases 0.000 description 1
- 150000008163 sugars Chemical class 0.000 description 1
- MVGSNCBCUWPVDA-MFOYZWKCSA-N sulindac sulfone Chemical compound CC1=C(CC(O)=O)C2=CC(F)=CC=C2\C1=C/C1=CC=C(S(C)(=O)=O)C=C1 MVGSNCBCUWPVDA-MFOYZWKCSA-N 0.000 description 1
- 235000012751 sunset yellow FCF Nutrition 0.000 description 1
- 239000004173 sunset yellow FCF Substances 0.000 description 1
- 230000008093 supporting effect Effects 0.000 description 1
- 239000000829 suppository Substances 0.000 description 1
- 230000001629 suppression Effects 0.000 description 1
- 239000000375 suspending agent Substances 0.000 description 1
- 230000007474 system interaction Effects 0.000 description 1
- 230000001839 systemic circulation Effects 0.000 description 1
- 238000009121 systemic therapy Methods 0.000 description 1
- 230000006794 tachycardia Effects 0.000 description 1
- 229950005890 tariquidar Drugs 0.000 description 1
- 235000012756 tartrazine Nutrition 0.000 description 1
- 239000004149 tartrazine Substances 0.000 description 1
- WBWWGRHZICKQGZ-GIHLXUJPSA-N taurocholic acid Chemical compound C([C@@H]1C[C@H]2O)[C@@H](O)CC[C@]1(C)[C@@H]1[C@@H]2[C@@H]2CC[C@@H]([C@@H](CCC(=O)NCCS(O)(=O)=O)C)[C@@]2(C)[C@H](O)C1 WBWWGRHZICKQGZ-GIHLXUJPSA-N 0.000 description 1
- DKPFODGZWDEEBT-QFIAKTPHSA-N taxane Chemical class C([C@]1(C)CCC[C@@H](C)[C@H]1C1)C[C@H]2[C@H](C)CC[C@@H]1C2(C)C DKPFODGZWDEEBT-QFIAKTPHSA-N 0.000 description 1
- RCINICONZNJXQF-MZXODVADSA-N taxol Chemical compound O([C@@H]1[C@@]2(C[C@@H](C(C)=C(C2(C)C)[C@H](C([C@]2(C)[C@@H](O)C[C@H]3OC[C@]3([C@H]21)OC(C)=O)=O)OC(=O)C)OC(=O)[C@H](O)[C@@H](NC(=O)C=1C=CC=CC=1)C=1C=CC=CC=1)O)C(=O)C1=CC=CC=C1 RCINICONZNJXQF-MZXODVADSA-N 0.000 description 1
- 230000004489 tear production Effects 0.000 description 1
- 230000002123 temporal effect Effects 0.000 description 1
- 231100000211 teratogenicity Toxicity 0.000 description 1
- 229960005353 testolactone Drugs 0.000 description 1
- BPEWUONYVDABNZ-DZBHQSCQSA-N testolactone Chemical compound O=C1C=C[C@]2(C)[C@H]3CC[C@](C)(OC(=O)CC4)[C@@H]4[C@@H]3CCC2=C1 BPEWUONYVDABNZ-DZBHQSCQSA-N 0.000 description 1
- 229960002372 tetracaine Drugs 0.000 description 1
- GKCBAIGFKIBETG-UHFFFAOYSA-N tetracaine Chemical compound CCCCNC1=CC=C(C(=O)OCCN(C)C)C=C1 GKCBAIGFKIBETG-UHFFFAOYSA-N 0.000 description 1
- 229960002180 tetracycline Drugs 0.000 description 1
- 229930101283 tetracycline Natural products 0.000 description 1
- 235000019364 tetracycline Nutrition 0.000 description 1
- 150000003522 tetracyclines Chemical class 0.000 description 1
- 238000011287 therapeutic dose Methods 0.000 description 1
- 230000008719 thickening Effects 0.000 description 1
- 229960001196 thiotepa Drugs 0.000 description 1
- 201000005060 thrombophlebitis Diseases 0.000 description 1
- 208000021510 thyroid gland disease Diseases 0.000 description 1
- 239000005495 thyroid hormone Substances 0.000 description 1
- 229940036555 thyroid hormone Drugs 0.000 description 1
- 210000001578 tight junction Anatomy 0.000 description 1
- 229960003087 tioguanine Drugs 0.000 description 1
- MNRILEROXIRVNJ-UHFFFAOYSA-N tioguanine Chemical compound N1C(N)=NC(=S)C2=NC=N[C]21 MNRILEROXIRVNJ-UHFFFAOYSA-N 0.000 description 1
- 229930003799 tocopherol Natural products 0.000 description 1
- 235000010384 tocopherol Nutrition 0.000 description 1
- 229960001295 tocopherol Drugs 0.000 description 1
- 239000011732 tocopherol Substances 0.000 description 1
- FUSNMLFNXJSCDI-UHFFFAOYSA-N tolnaftate Chemical compound C=1C=C2C=CC=CC2=CC=1OC(=S)N(C)C1=CC=CC(C)=C1 FUSNMLFNXJSCDI-UHFFFAOYSA-N 0.000 description 1
- 229960004880 tolnaftate Drugs 0.000 description 1
- JOXIMZWYDAKGHI-UHFFFAOYSA-N toluene-4-sulfonic acid Chemical compound CC1=CC=C(S(O)(=O)=O)C=C1 JOXIMZWYDAKGHI-UHFFFAOYSA-N 0.000 description 1
- GYHCTFXIZSNGJT-UHFFFAOYSA-N tolvaptan Chemical compound CC1=CC=CC=C1C(=O)NC(C=C1C)=CC=C1C(=O)N1C2=CC=C(Cl)C=C2C(O)CCC1 GYHCTFXIZSNGJT-UHFFFAOYSA-N 0.000 description 1
- 229960001256 tolvaptan Drugs 0.000 description 1
- 229960000303 topotecan Drugs 0.000 description 1
- UCFGDBYHRUNTLO-QHCPKHFHSA-N topotecan Chemical compound C1=C(O)C(CN(C)C)=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 UCFGDBYHRUNTLO-QHCPKHFHSA-N 0.000 description 1
- 231100000765 toxin Toxicity 0.000 description 1
- 108700012359 toxins Proteins 0.000 description 1
- PKVRCIRHQMSYJX-AIFWHQITSA-N trabectedin Chemical compound C([C@@]1(C(OC2)=O)NCCC3=C1C=C(C(=C3)O)OC)S[C@@H]1C3=C(OC(C)=O)C(C)=C4OCOC4=C3[C@H]2N2[C@@H](O)[C@H](CC=3C4=C(O)C(OC)=C(C)C=3)N(C)[C@H]4[C@@H]21 PKVRCIRHQMSYJX-AIFWHQITSA-N 0.000 description 1
- 229960000977 trabectedin Drugs 0.000 description 1
- QQJLHRRUATVHED-UHFFFAOYSA-N tramazoline Chemical compound N1CCN=C1NC1=CC=CC2=C1CCCC2 QQJLHRRUATVHED-UHFFFAOYSA-N 0.000 description 1
- 229960001262 tramazoline Drugs 0.000 description 1
- 230000002103 transcriptional effect Effects 0.000 description 1
- 230000002463 transducing effect Effects 0.000 description 1
- 229960001727 tretinoin Drugs 0.000 description 1
- QORWJWZARLRLPR-UHFFFAOYSA-H tricalcium bis(phosphate) Chemical compound [Ca+2].[Ca+2].[Ca+2].[O-]P([O-])([O-])=O.[O-]P([O-])([O-])=O QORWJWZARLRLPR-UHFFFAOYSA-H 0.000 description 1
- 229940078499 tricalcium phosphate Drugs 0.000 description 1
- 229910000391 tricalcium phosphate Inorganic materials 0.000 description 1
- 235000019731 tricalcium phosphate Nutrition 0.000 description 1
- 239000003029 tricyclic antidepressant agent Substances 0.000 description 1
- 210000003901 trigeminal nerve Anatomy 0.000 description 1
- 230000001960 triggered effect Effects 0.000 description 1
- 239000013638 trimer Substances 0.000 description 1
- 229960004418 trolamine Drugs 0.000 description 1
- 229950010147 troxacitabine Drugs 0.000 description 1
- RXRGZNYSEHTMHC-BQBZGAKWSA-N troxacitabine Chemical compound O=C1N=C(N)C=CN1[C@H]1O[C@@H](CO)OC1 RXRGZNYSEHTMHC-BQBZGAKWSA-N 0.000 description 1
- 239000002447 tumor necrosis factor alpha converting enzyme inhibitor Substances 0.000 description 1
- 229920001664 tyloxapol Polymers 0.000 description 1
- MDYZKJNTKZIUSK-UHFFFAOYSA-N tyloxapol Chemical compound O=C.C1CO1.CC(C)(C)CC(C)(C)C1=CC=C(O)C=C1 MDYZKJNTKZIUSK-UHFFFAOYSA-N 0.000 description 1
- 229960004224 tyloxapol Drugs 0.000 description 1
- 230000034512 ubiquitination Effects 0.000 description 1
- 238000010798 ubiquitination Methods 0.000 description 1
- 231100000397 ulcer Toxicity 0.000 description 1
- 238000011144 upstream manufacturing Methods 0.000 description 1
- 229940035893 uracil Drugs 0.000 description 1
- 229960001055 uracil mustard Drugs 0.000 description 1
- 230000003424 uricosuric effect Effects 0.000 description 1
- 208000019206 urinary tract infection Diseases 0.000 description 1
- 229940093257 valacyclovir Drugs 0.000 description 1
- ZOCKGBMQLCSHFP-KQRAQHLDSA-N valrubicin Chemical compound O([C@H]1C[C@](CC2=C(O)C=3C(=O)C4=CC=CC(OC)=C4C(=O)C=3C(O)=C21)(O)C(=O)COC(=O)CCCC)[C@H]1C[C@H](NC(=O)C(F)(F)F)[C@H](O)[C@H](C)O1 ZOCKGBMQLCSHFP-KQRAQHLDSA-N 0.000 description 1
- 229960000653 valrubicin Drugs 0.000 description 1
- 230000002792 vascular Effects 0.000 description 1
- 208000019553 vascular disease Diseases 0.000 description 1
- 230000006442 vascular tone Effects 0.000 description 1
- 235000015112 vegetable and seed oil Nutrition 0.000 description 1
- 239000008158 vegetable oil Substances 0.000 description 1
- 239000003981 vehicle Substances 0.000 description 1
- 210000003462 vein Anatomy 0.000 description 1
- 231100000925 very toxic Toxicity 0.000 description 1
- 210000004721 vestibular dark cell Anatomy 0.000 description 1
- 208000027491 vestibular disease Diseases 0.000 description 1
- 229960003048 vinblastine Drugs 0.000 description 1
- JXLYSJRDGCGARV-XQKSVPLYSA-N vincaleukoblastine Chemical compound C([C@@H](C[C@]1(C(=O)OC)C=2C(=CC3=C([C@]45[C@H]([C@@]([C@H](OC(C)=O)[C@]6(CC)C=CCN([C@H]56)CC4)(O)C(=O)OC)N3C)C=2)OC)C[C@@](C2)(O)CC)N2CCC2=C1NC1=CC=CC=C21 JXLYSJRDGCGARV-XQKSVPLYSA-N 0.000 description 1
- GBABOYUKABKIAF-GHYRFKGUSA-N vinorelbine Chemical compound C1N(CC=2C3=CC=CC=C3NC=22)CC(CC)=C[C@H]1C[C@]2(C(=O)OC)C1=CC([C@]23[C@H]([C@]([C@H](OC(C)=O)[C@]4(CC)C=CCN([C@H]34)CC2)(O)C(=O)OC)N2C)=C2C=C1OC GBABOYUKABKIAF-GHYRFKGUSA-N 0.000 description 1
- 229960002066 vinorelbine Drugs 0.000 description 1
- 238000007794 visualization technique Methods 0.000 description 1
- WAEXFXRVDQXREF-UHFFFAOYSA-N vorinostat Chemical compound ONC(=O)CCCCCCC(=O)NC1=CC=CC=C1 WAEXFXRVDQXREF-UHFFFAOYSA-N 0.000 description 1
- 229960000237 vorinostat Drugs 0.000 description 1
- 230000003442 weekly effect Effects 0.000 description 1
- 238000009736 wetting Methods 0.000 description 1
- 229940002639 xalatan Drugs 0.000 description 1
- 235000010493 xanthan gum Nutrition 0.000 description 1
- 239000000230 xanthan gum Substances 0.000 description 1
- 229940082509 xanthan gum Drugs 0.000 description 1
- UHVMMEOXYDMDKI-JKYCWFKZSA-L zinc;1-(5-cyanopyridin-2-yl)-3-[(1s,2s)-2-(6-fluoro-2-hydroxy-3-propanoylphenyl)cyclopropyl]urea;diacetate Chemical compound [Zn+2].CC([O-])=O.CC([O-])=O.CCC(=O)C1=CC=C(F)C([C@H]2[C@H](C2)NC(=O)NC=2N=CC(=CC=2)C#N)=C1O UHVMMEOXYDMDKI-JKYCWFKZSA-L 0.000 description 1
- 229950005752 zosuquidar Drugs 0.000 description 1
- GVJHHUAWPYXKBD-IEOSBIPESA-N α-tocopherol Chemical compound OC1=C(C)C(C)=C2O[C@@](CCC[C@H](C)CCC[C@H](C)CCCC(C)C)(C)CCC2=C1C GVJHHUAWPYXKBD-IEOSBIPESA-N 0.000 description 1
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/30—Macromolecular organic or inorganic compounds, e.g. inorganic polyphosphates
- A61K47/34—Macromolecular compounds obtained otherwise than by reactions only involving carbon-to-carbon unsaturated bonds, e.g. polyesters, polyamino acids, polysiloxanes, polyphosphazines, copolymers of polyalkylene glycol or poloxamers
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/045—Hydroxy compounds, e.g. alcohols; Salts thereof, e.g. alcoholates
- A61K31/05—Phenols
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
- A61K31/135—Amines having aromatic rings, e.g. ketamine, nortriptyline
- A61K31/137—Arylalkylamines, e.g. amphetamine, epinephrine, salbutamol, ephedrine or methadone
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/325—Carbamic acids; Thiocarbamic acids; Anhydrides or salts thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/41—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having five-membered rings with two or more ring hetero atoms, at least one of which being nitrogen, e.g. tetrazole
- A61K31/425—Thiazoles
- A61K31/429—Thiazoles condensed with heterocyclic ring systems
- A61K31/43—Compounds containing 4-thia-1-azabicyclo [3.2.0] heptane ring systems, i.e. compounds containing a ring system of the formula, e.g. penicillins, penems
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/4353—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom ortho- or peri-condensed with heterocyclic ring systems
- A61K31/436—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom ortho- or peri-condensed with heterocyclic ring systems the heterocyclic ring system containing a six-membered ring having oxygen as a ring hetero atom, e.g. rapamycin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/505—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim
- A61K31/519—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim ortho- or peri-condensed with heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/55—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole
- A61K31/551—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole having two nitrogen atoms, e.g. dilazep
- A61K31/5513—1,4-Benzodiazepines, e.g. diazepam or clozapine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/55—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole
- A61K31/551—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having seven-membered rings, e.g. azelastine, pentylenetetrazole having two nitrogen atoms, e.g. dilazep
- A61K31/5513—1,4-Benzodiazepines, e.g. diazepam or clozapine
- A61K31/5517—1,4-Benzodiazepines, e.g. diazepam or clozapine condensed with five-membered rings having nitrogen as a ring hetero atom, e.g. imidazobenzodiazepines, triazolam
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
- A61K38/1808—Epidermal growth factor [EGF] urogastrone
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
- A61K38/1825—Fibroblast growth factor [FGF]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
- A61K38/185—Nerve growth factor [NGF]; Brain derived neurotrophic factor [BDNF]; Ciliary neurotrophic factor [CNTF]; Glial derived neurotrophic factor [GDNF]; Neurotrophins, e.g. NT-3
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
- A61K38/1858—Platelet-derived growth factor [PDGF]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/18—Growth factors; Growth regulators
- A61K38/1883—Neuregulins, e.g.. p185erbB2 ligands, glial growth factor, heregulin, ARIA, neu differentiation factor
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/08—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing oxygen, e.g. ethers, acetals, ketones, quinones, aldehydes, peroxides
- A61K47/14—Esters of carboxylic acids, e.g. fatty acid monoglycerides, medium-chain triglycerides, parabens or PEG fatty acid esters
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/16—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing nitrogen, e.g. nitro-, nitroso-, azo-compounds, nitriles, cyanates
- A61K47/18—Amines; Amides; Ureas; Quaternary ammonium compounds; Amino acids; Oligopeptides having up to five amino acids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/30—Macromolecular organic or inorganic compounds, e.g. inorganic polyphosphates
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/30—Macromolecular organic or inorganic compounds, e.g. inorganic polyphosphates
- A61K47/32—Macromolecular compounds obtained by reactions only involving carbon-to-carbon unsaturated bonds, e.g. carbomers, poly(meth)acrylates, or polyvinyl pyrrolidone
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/30—Macromolecular organic or inorganic compounds, e.g. inorganic polyphosphates
- A61K47/36—Polysaccharides; Derivatives thereof, e.g. gums, starch, alginate, dextrin, hyaluronic acid, chitosan, inulin, agar or pectin
- A61K47/38—Cellulose; Derivatives thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0046—Ear
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/06—Ointments; Bases therefor; Other semi-solid forms, e.g. creams, sticks, gels
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/10—Dispersions; Emulsions
- A61K9/127—Liposomes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
- A61K9/16—Agglomerates; Granulates; Microbeadlets ; Microspheres; Pellets; Solid products obtained by spray drying, spray freeze drying, spray congealing,(multiple) emulsion solvent evaporation or extraction
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/02—Drugs for disorders of the nervous system for peripheral neuropathies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/22—Anxiolytics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P27/00—Drugs for disorders of the senses
- A61P27/16—Otologicals
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P31/00—Antiinfectives, i.e. antibiotics, antiseptics, chemotherapeutics
- A61P31/04—Antibacterial agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P37/00—Drugs for immunological or allergic disorders
- A61P37/02—Immunomodulators
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P43/00—Drugs for specific purposes, not provided for in groups A61P1/00-A61P41/00
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/24—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against cytokines, lymphokines or interferons
- C07K16/241—Tumor Necrosis Factors
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/21—Immunoglobulins specific features characterized by taxonomic origin from primates, e.g. man
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/70—Immunoglobulins specific features characterized by effect upon binding to a cell or to an antigen
- C07K2317/76—Antagonist effect on antigen, e.g. neutralization or inhibition of binding
Definitions
- formulations for enhanced drug delivery into the external, middle and/or inner ear including the cochlea and vestibular labyrinth; preferably with little or no systemic release of the drug.
- the environment of the inner ear is an isolated environment.
- the endolymph and the perilymph are static fluids and are not in contiguous contact with the circulatory system.
- the blood - labyrinth - barrier (BLS), which includes a blood-endolymph barrier and a blood-perilymph barrier, consists of tight junctions between specialized epithelial cells in the labyrinth spaces (i.e., the vestibular and cochlear spaces).
- active agents e.g., immunomoduiators, aural pressure modulators, antimicrobials
- Auris hair cells are bathed in endolymphatic or perilymphatic fluids and cochlear recycling of potassium ions is important for hair cell function.
- the inner ear When the inner ear is infected, there is an influx of leukocytes and/or immtinoglobins (e.g. in response to a microbial infection) into the endolymph and/or the perilymph and the delicate ionic composition of inner car fluids is upset by the influx of leukocytes and/or immunoglobins.
- a change in the ionic composition of inner ear fluids results in hearing loss, loss of balance and/or ossification of auditory structures.
- a ⁇ ris formulations Due to the susceptibilty of the inner ear to infections, a ⁇ ris formulations require a level of sterility that has not been recognized hitherto in prior art.
- auris formulations that are sterilized with stringent sterilty requirements and are suitable for administration to the middle and/or inner ear.
- the auris compatible compositions described herein are substantially free of pyrogens and/or microbes.
- otic formulations with an ionic balance that is compatible with the perilymph and/or the endolympb. and does not cause any change in cochlear potential.
- osmoiariiy/osruolality of the present formulations is adjusted, for example, by the use of appropriate salt concentrations ⁇ e.g, , concentration of sodium salts) or the use of tonicity agents which renders the formulations endolymph-compatible and/or perilymph-cornpatibie (i.e. isotonic with the endolymph and/or perilymph).
- the endolymph-compatible and/or peri lymph-compatible formulations described herein cause minimal disturbance to the environment of the inner ear and cause minimum discomfort (e.g, vertigo) to a mammal (e.g., a human) upon adminstration.
- the formulations comprise polymers that are biodegradable and/or dispersable, and/or otherwise non-toxic to the inner ear environment.
- the fo ⁇ nulations described herein are free of preservatives and cause minimal disturbance (e.g., change in pH or osmolality, irritation) in auditor)' structures.
- the formulations described herein comprise antioxidants that are non-irritating and/or non-toxic to otic structures.
- auris formulations described herein are controlled release formulations, and are administered at reduced dosing frequency compared to the current standard of care.
- a reduced frequency of administration alleviates discomfort caused by multiple intratympanic injections in individuals undergoing treatment for a middle and/or inner ear disease, disorder or condition.
- a reduced frequency of administration of intratympanic injections reduces the risk of permanent damage (e.g., perforation) to the ear drum.
- the formulations described herein provide a constant, sustained, extended, delayed or pulsatile rate of release of an active agent into the inner car environment and thus avoid any variability in drug exposure in treatment of otic disorders.
- a ⁇ ris formulations described herein are administered into the ear canal, or in the vestibule of the ear. Access to, for example, the vestibular and cochlear apparatus will occur through the auri$ media including the round window membrane, the oval window/stapes footplate, the annular ligament and through the otic capsule/temporal bone. Otic administration of the formulations described herein avoids toxicity associated with systemic administration (e.g., hepatotoxicity, cardiotoxicity, gastrointestinal side effects, renal toxicity) of the active agents. In some instances, localized administration in the ear allows an active agent to reach a target organ (e.g., inner ear) in the absence of systemic accumulation of the active agent. In some instances, local administration to the ear provides a higher therapeutic index for an active agent that would otherwise have dose- limiting systemic toxicity.
- systemic administration e.g., hepatotoxicity, cardiotoxicity, gastrointestinal side effects, renal toxicity
- a disadvantage of liquid formulations is their propensity to drip into the eustachian tube and cause rapid clearance of the formulation from the inner ear.
- a ⁇ ris formulations comprising polymers that gel at body temperature and remain in contact with the target auditory surfaces (e.g., the round window) for extended periods of time.
- the fomulations further comprise mucoadhesives that allow the formulations to adhere to otic mucosal surfaces,
- the auris formulations described herein avoid attenuation of therapeutic benefit due to drainage or leakage of active agents via the eustachian tube.
- compositions for use in the treatment of an otic disease or condition formulated to provide a therapeutically effective amount of an imm ⁇ nomodulating agent across the round window membrane into the cochlea, the formulation comprising:
- the pharmaceutical formulation has a perilymph-suitable osmolarity between about 250 and 320 mOsm/L
- jOOl 11 Provided herein, in some embodiments, are pharmaceutical formulations tor use in the treatment of an otic disease or condition formulated to provide a therapeutically effective amount of an immunomodulating agent across the round window membrane into the cochlea, the formulation comprising:
- an immunomodulating agent between about 0.1 mg/niL to about 70 mg''mL of an immunomodulating agent, or pharmaceutically acceptable prodrug or salt thereof;
- the pharmaceutical formulation lias a perilymph-suitable osmolality between about 250 and 320 mOsm/L,
- cfii colony forming units of microbiological agents per grain of formulation
- RU endotoxin units
- the immunor ⁇ oduiattng agent is released from the formulation for a period of at least 3 days.
- the pharmaceutical formulation is an auris- acceptable therraoreversible gel.
- the poiyoxyelhylene-polyoxypropylene triblock copolymer is biodegradable,
- the formulations further comprise a mucoadhesive.
- the formulations further comprise a penetration enhancer.
- the formulations further comprise a thickening agent.
- the formulations further comprise a dye.
- formulations further comprising a drug delivery device selected from a needle and syringe, a pump, a microinjection device, a wick, an in situ forming spongy material or combinations thereof.
- the immunomodulating agent is ⁇ i the form of a free base, salt, a prodrug, or a combination thereof.
- the irnmuoomodulating agent comprises multiparticulates.
- immunomodulating agent is essentially iu the form of micronized particles.
- the immunomodulating agent is an anli-TNF agent, a calcineurin inhibitor, an IKK inhibitor, an interleukin inhibitor, a TNF-a converting enzyme (TACK) inhibitor, or a loll-like receptor inhibitor.
- the formulations further comprise an immunomodulating agent, or pharmaceutically acceptable salt thereof, as an immediate release agent.
- the formulations described herein further comprise au additional therapeutic agent.
- the additional therapeutic agent is a Na/K ATPase modulator, a chemotherapeutic agent, a collagen, a gamma-globulin, an interferon, art anti-microbial agent, an antibiotic, a local acting anesthetic agent, a platelet activator factor antagonist, a nitric oxide synthase inhibitor, an anti-vertigo agent, a vasopressin antagonist, an anti-viral, an anti-emetic agent or combinations thereof.
- the pH of the composition is between about 6.0 to about 7.6.
- the ratio of a polyoxyelhylene-polyoxypropyle ⁇ e triblock copolymer of general formula El 06 P70 El 06 to a thickening agent is from about 40: 1 to about 10: 1.
- the thickening agent is carboxymethyl cellulose.
- the otic disease or condition is Meniere's disease, sudden sensorineural hearing loss, noise induced hearing loss, age-related hearing loss, auto immune ear disease or tinnitus.
- Also provided herein is a method of treating an otic disease or condition comprising administering to an individual in need thereof an intratympanic composition comprising
- the pharmaceutical formulation has a perilymph-suitable osmolarity between about 250 and 320 mOsrn/L,
- the immunomodulating agent is an anti-TNF agent, a caicineurin inhibitor, an IKK inhibitor, an interleukin inhibitor, a TNF-a convening enzyme (TACE) inhibitor, or a toll-like receptor inhibitor.
- TACE TNF-a convening enzyme
- the immunomodulating agent is released from the composition for a period of at least 3 days.
- the composition is administered across the round window.
- the otic disease or condition is Meniere's disease, sudden sensorineural hearing loss, age-related hearing loss, noise induced hearing loss, auto immune ear disease or tinnitus.
- compositions for use in the treatment of an otic disease or condition formulated to provide a therapeutically effective amount of an aural pressure modulating agent across the round window membrane into the cochlea, the formulation comprising:
- an aural pressure modulating agent between about 0.2% to about 6% by weight of an aural pressure modulating agent, or pharmaceutically acceptable prodrug or salt thereof;
- the pharmaceutical formulation has a perilymph-suitable osmolality between about 250 and 320 mOsm/L
- arc pharmaceutical formulations for use in the treatment of an otic disease or condition formulated to provide a therapeutically effective amount of an aural pressure modulating agent across the round window membrane into the cochlea, the fonriuiation comprising:
- aural pressure modulating agent between about 0.1 mg/mL to about 70 mg/mL of art aural pressure modulating agent, or pharmaceutically acceptable prodrug or salt (hereof;
- the pharmaceutical formulation has a perilymph-suitable osmolality between, about 250 and 320 m ⁇ sm/l.
- the aural pressure modulating agent is released from the formulation for a period of at least 3 days.
- the pharmaceutical formulation is an auris- acceptable thermoreversiblc gel.
- the polyoxyethylene-polyoxypropylenc triblock copolymer is biodegradable.
- the formulations further comprise a round window membrane mucoadhesive.
- the formulations further comprise a round window membrane penetration enhancer.
- the formulations further comprise thickening agent.
- the formulations further comprise a dye.
- the formulations further comprise a drug delivery device selected from a needle and syringe, a pump, a microinjection device, a wick, an in situ forming spongy material or combinations thereof.
- the aural pressure modulating agent has limited or no systemic release, systemic toxicity, poor PK characteristics, or combinations thereof.
- the aural pressure modulating agent is administered in the form of a free base, salt, a prodrug, or a combination thereof.
- the aural pressure modulating agent comprises multiparticulates.
- the aural pressure modulating agent is essentially in the form of micronized particles.
- the aural pressure modulating agent is a modulator of aquaporin, an estrogen related receptor beta modulator, a gap junction protein modulator, an NMDA receptor modulator, an osmotic diuretic, a progesterone receptor modulator, a prostaglandin modulator, or a vasopressin receptor modulator.
- the formulations described herein further comprise an aural pressure modulating agent, or pharmaceutically acceptable salt thereof, as an immediate release agent.
- the formulations described herein further comprise an additional therapeutic agent.
- the additional therapeutic agent is Na/K ATPase modulator, a chemotherapeutic agent, a collagen, a gamma-globuliu, an interferon, an anti-microbial agent, an antibiotic, a local acting anesthetic agent, a platelet activator factor antagonist, a nitric oxide synthase inhibitor, an anti-vertigo medicine, a vasopressin antagonist, an anti-viral, an anti- emetic agent or combinations thereof.
- the pH of the composition is between about 6.0 to about 7.6.
- (he ratio of a polyoxyethylene-polyoxypropylene triblock copolymer of general fonnula El 06 P70 E106 to a thickening agent is from about 40:1 to about 10:1.
- the thickening agent is carboxymethyl cellulose.
- the otic disease or condition is Meniere's disease, sudden sensorineural hearing loss, age-related hearing loss, noise induced hearing loss, auto immune ear disease or tinnitus.
- a method of treating an otic disease or condition comprising administering to an individual in need thereof an intralympanic composition comprising between about 0.2% Io about 6% by weight of an aural pressure modulating agent or pharmaceutically acceptable prodrug or salt thereof;
- the pharmaceutical formulation has a perilymph-suitable osmolality between about 250 and 320 mOsm/L
- the aural pressure modulating agent is a modulator of aquaporin.
- an estrogen related receptor beta modulator a gap junction protein modulator, an NMDA receptor modulator, an osmotic diuretic, a progesterone receptor modulator, a prostaglandin modulator, or a vasopressin receptor modulator.
- the aural pressure modulating agent is released from the composition for a period of at least 3 days, ⁇ n some embodiments of (he method, the composition is administered across the round window.
- the otic disease or condition is Meniere's disease, sudden sensorineural hearing loss, age-related hearing loss, noise induced hearing ioss, auto immune ear disease or tinnitus.
- the term '"subtantially low degradation products means less than 5% by weight of the active agent are degradation products of the active agent. In further embodiments, the term means less than 3% by weight of the active agent are degradation products of the active agent. In yet further embodiments, the term means less than 2% by weight of the active agent are degradation products of the active agent. In further embodiments, the term means less than I % by weight of the active agent are degradation products of the active agent.
- Figure 1 illustrates a comparison of non-sustained release formulations and sustained release formulations.
- Figure 2 illustrates the effect of concentration on viscosity of aqueous solutions of Blanos refined CMC
- Figure 3 illustrates the effect of concentration on viscosity of aqueous solutions of
- Systemic administration of active agents is, in some instances, ineffectual in the treatment of diseases that affect inner ear structures.
- the cochlear canals and the cochlea are isolated from the circulatory system limiting systemic delivery of active agents to target sites in the inner ear.
- systemic drug administration creates a potential inequality in drug concentration with higher circulating levels in the serum, and lower levels in the target auris interna organ structures. Jn certain instances, large amounts of drug are required to overcome this inequality in order to deliver sufficient, therapeutically effective quantities of a drug to auditory structures.
- systemic drug administration also increases the likelihood of secondary systemic accumulation and consequent adverse side effects.
- Currently available treatment for inner ear diseases also carries the risk of attendant side effects.
- available methods require multiple daily doses (e.g., intratympanic injection or infusion) of drugs.
- multiple daily intratympanic injections cause patient discomfort and non-compliance.
- delivery of active agents to the inner ear via otic drops administered in the ear canal or via intratyrapanic injection is hindered by the biological barrier presented by the blood-labyrinth-barrier (BLB), the oval window membrane and/or the round window membrane.
- BLB blood-labyrinth-barrier
- delivery of active agents to the inner ear via otic drops or intratympanic injection causes osmotic imbalance in inner ear structures, introduces infections or other immune disorders as a result of microbial or endotoxin presence, or results in permanent structural damage (e.g. perforation of the tympanic membrane), resulting in hearing loss and the like.
- U.S. Application Publication Nos. 2006/0063802 and 2005/0214338 disclose compositions comprising arylcycloalkylamine NMDA antagonists for local administration to the inner ear. There is no disclosure of controlled release formulations, osmolarily or pH requirements, or sterility requirements for the compositions.
- WO 2007/038949 discloses compositions comprising arylcycloalkylamiiie NMDA antagonists in the treatment of inner ear disorders. No guidance is provided on pyrogenicity, sterility requirements, viscosity levels and/or controlled release characteristics of the formulation.
- Fernandez et al. Biornateriah, 26: 3311-3318 (2005) describes compositions which comprise prednisolone useful to treat inner ear disease such as Meniere's disease. Fernandez et al. do not disclose osmolarily, pyrogenicity, pH, or sterility levels of the compositions described therein. Paulson et al. The Laryngoscope, 1 18: 706 (2008) describe sustained release compositions which comprise dexamethasone useful in treatment of, inter alia, inner ear diseases such as
- lntratympauic injection of therapeutic agents is the technique of injecting a Iherapeutic agent behind the tympanic membrane into the auris media and/or auris interna.
- auris media and/or auris interna some challenges do remain. For example, access to the round window membrane, the site of drug absorption into the auris interna, can be challenging.
- intra-tympanie injections create several unrecognized problems not addressed by currently available treatment regimens, such as changing the osmolarity and pH of the perilymph artd endolymph. and introducing pathogens and endotoxins that directly or indirectly damage inner ear structures.
- One of the reasons the art may not have recognized these problems is that there are no approved intra-tympanic compositions: the inner ear provides sui generis formulation challenges.
- compositions developed for other parts of the body have little to no relevance for an intra- lympanic composition.
- otic formulations that meet stringent criteria for pH, osmolality, ionic balance, sterility, endotoxin and/or pyrogen levels.
- the auris compositions described herein are compatible with the microenvironrnent of the inner ear (e.g., the perilymph) and are suitable for administration to humaus.
- the formulations described herein comprise dyes and aid visualization of the administered compositions obviating the need for invasive procedures (e.g., removal of perilymph) during preclinical and/or clinical development of intratympanic therapeutics.
- auris- acceptable formulations and compositions that locally treat auris target structures and provide extended exposure of otic active agents to the target auris structures.
- the auris formulations described herein are polymer based formulations designed for stringent osmolarity and pH ranges that are compatible with auditory structures aud/or the endolymph and perilymph.
- the formulations described herein are controlled release formulations that provide extended release tor a period of at least 3 days and meet stringent sterility requirements.
- otic compositions described herein contain lower endotoxin levels (e.g.
- the otic formulations described herein contain low levels of colony forming units (e.g., ⁇ 50 CFUs) per gram of the formulation.
- the auris formulations described herein are substantially free of pyrogens and/or microbes.
- the auris formulations described herein are formulated to preserve the ionic balance of the endolymph and/or the perilymph. The stringent requirement for sterility and compatibility with inner ear fluids for otic formulations lias not been addressed hereto.
- the formulations described herein represent an advantage over currently available therapeutics because they are sterile controlled release otic fomulations tliat are compatible with auris stmcutures (e.g., the perilymph) and are safe for long term administration to humans in need thereof.
- auris stmcutures e.g., the perilymph
- the formulations described herein prevent an initial burst release upon administration to the inner ear; i.e., the formulations avoid causing a dramatic change in the pH of the endolymph or perilymph and subsequently reduce the impact on balance and/or hearing upon administration.
- the locally applied auris-acceptable formulations and compositions described herein are compatible with auris structures, and administered either directly to the desired auris structure, e.g. the cochlear region, or administered to a structure in direct communication with areas of the auris structure; in the case of the cochlear region, for example, including but not limittxl to the round window membrane, the crista fenestrae cochleae or (he oval window membrane.
- an advantage of the controlled release formulations described herein is that they provide a constant rate of release of a drug from the formulation and provide a constant prolonged source of exposure of an otic active agent to the inner ear of an individual or patient suffering from an otic disorder, reducing or eliminating any variabilities associated with other methods of treatment (such as, e.g., otic drops and/or multiple intratympanic injections),
- the drug formulations described herein provide extended release of the active ingredient(s) into the middle and/or inner ear (auris interna), including the cochlea and vestibular labyrinth.
- a further option includes an immediate or rapid release component in combination with a controlled release component.
- auris-acceptable with respect to a formulation, composition or ingredient, as used herein, includes having no persistent detrimental effect on the auris media (or middle ear) and the auris interna (or inner ear) of the subject being treated.
- v 'auris-phannaceuticaliy acceptable refers to a material, such as a carrier or diluent, which does not abrogate the biological activity or properties of the compound in reference to the auris media (or middle ear) and the auris interna ⁇ or inner ear), and is relatively or is reduced in toxicity to the auris media (or middle ear) and the auris interna (or inner ear), i.e., the material is administered to an individual without causing undesirable biological effects or interacting in a deleterious manner with any of the components of the composition in which it is contained.
- amelioration or lessening of the symptoms of a particular otic disease, disorder or condition by administration of a particular compound or pharmaceutical composition refers to any decrease of severity, delay in onset, slowing of progression, or shortening of duration, whether permanent or temporary, lasting or transient that is attributed io or associated with administration of the compound or composition.
- immunomodulator agent or “immune-modulating agent” are used as synonyms.
- anti lumor necrosis factor agent or "TNF modulator” or “TNF modulating agent * ' or "TNF-alpha modulator” or "anti-TNF alpha agenf are used as synonyms.
- anti-TNF agent and its synonyms generally refer to agents that counteract the biological effect of TNF- ⁇ or the biological effect of pro-TNF- ⁇ stimulus including agents which bind to and antagonize the molecular target: here, tumor necrosis factor alpha or TNF-alpha (TNF- Oc), agents which inhibit release of TNF- ⁇ , or agents which interfere with TNF- ⁇ gene expression due to pro-TNF- ⁇ stimulus. Also included are agents that indirectly antagonize the biological activity of TNF- ⁇ by modulating targets in the general pathway of TNF- ⁇ . activation, including but not limited to targets upstream of the pathway of TNF-alpha activation, including but not limited to agents which increase TNF-alpha expression, activity or function.
- aural pressure modulating agent or "aural pressure modulator” are used as synonyms and do not define the degree of efficacy .
- the aural pressure modulator also includes compounds that modulate the expression or posMranscripiional processing of a fluid homeostasis protein, including vasopressin and estrogen-related receptor beta protein.
- vasopressin receptor or estrogen-related receptor beta modulators include compounds thai influence vasopressin receptor or estrogen-related receptor beta signalling or downstream functions under the control of the vasopressin receptor or estrogen-related receptor beta, such as aquaporin function.
- Vasopressin receptor or estrogen-related receptor beta modulating agents includes compounds that increase and/or decrease vasopressin receptor or estrogen-related receptor beta function, including antagonists, inhibitors, agonists, partial agonists and the like.
- Modulator of neuron and/or hair cells of the auris and “auris sensory cell modulating agent” are synonyms. They include agents that promote the growth and/or regeneration of neurons and/or the hair cells of the auris, and agents that destroy neurons and/or hair cells of the auris.
- antimicrobial agent refers to compounds that inhibit (lie growth, proliferation, or multiplication of microbes, or that kill microbes. Suitable “antimicrobial agents” are antibacterial agents (effective against bacteria), antiviral agents (effective against viruses), antifungal agents (effective against fungi), antiprotozoal (effective against protozoa), and/or antiparasitic to any class of microbial parasites. "Antimicrobial agents'- may work by any suitable mechanism against the microbes, including by being toxic or cytostatic.
- lite phrase "antimicrobial small molecule” refers to antimicrobial compounds that are of relatively low molecular weight, e.g., less than 1 ,000 molecular weight, that are effective for the treatment of otic disorders, particularly otic disorders caused by pathogenic microbes, and are suitable for use in the formulations disclosed herein. Suitable “antimicrobial small molecules” include antibacterial, antiviral, antifungal, antiprotozoal, and antiparasitic small molecules. [0066] "Modulator of free-radicals" and “free-radical modulating agent” are synonyms. They refer to agents that modulate the production of and/or damage caused by free radicals, especially reactive oxygen species.
- the terms '"ion channel modulating agent", “modulator of ion channels” or “ion channel modulator” are used as synonyms and do not define the degree of efficacy.
- the ion channel modulator also includes compounds that modulate the expression or post-transcriptional processing of a fluid homeostasis protein, including vasopressin and estrogen-related receptor beta protein.
- vasopressin receptor or estrogen-related receptor beta modulators include compounds that influence vasopressin receptor or estrogen-related receptor beta signalling or downstream functions under the control of the vasopressin receptor or estrogen-related receptor beta, such as aquaporin function.
- Vasopressin receptor or estrogen-related receptor beta modulating agents includes compounds that increase and/or decrease vasopressin receptor or estrogen-related receptor beta function, including antagonists, inhibitors, agonists, partial agonists and the like.
- otic agent or “otic structure modulating agent” or “otic therapeutic agent” or “otic active agent” or “active agent” refers to compounds that are effective for the treatment of otic disorders, e.g., otitis media, otosclerosis, autoimmune diseases of the ear and cancer of the ear, and are suitable for use in the formulations disclosed herein.
- Au “otic agent” or “otic structure modulating agent” or “otic therapeutic agent” or '"otic active agent” or “active agent” includes, but is not limited to, compounds that act as an agonist, a partial agonist, an antagonist, a partial antagonist, an inverse agonist, a competitive antagonist, a neutral antagonist, an orthosteric antagonist, an allosteric antagonist, or a positive aliosteric modulator of an otic structure modulating target, or combinations thereof.
- Body disorder refers to a disorder, illness, or condition which causes a subject to feel unsteady, or to have a sensation of movement, included in this definition are dizziness, vertigo, disequilibrium, and pre-syncope.
- Diseases which are classified as balance disorders include, but are not limited to, Ramsay Hunt's Syndrome, Meniere's Disease, mal de debarquement, benign paroxysmal positional vertigo, and labyrinthitis.
- CNS modulator and “CNS modulating agent ' ' are synonyms. They refer to agents that decrease, diminish, partially suppress, fully suppress, ameliorate, antagonize, agonize, stimulate or increase the activity of die CNS. For example, they may increase the activity of GABA by, for example, increasing the sensitivity of the GABA receptors, or they may alter the depolarization in neurons.
- “Local anesthetic” means a substance which causes a reversible loss of sensation and/or a loss of nociception. Often, these substances function by decreasing the rate of the depolarization and repolarization of excitable membranes (for example, neurons).
- local anesthetics include lidocaine, benzocaine, prilocaine, and tetracaine.
- Module of the GABA A receptor “modulator of the GABA receptor.”
- “GABA ⁇ receptor modulator,” and “OABA receptor modulator,'' are synonyms. They refer to substances which modulate the activity of die GABA neurotransmitter, by, for example, increasing the sensitivity of the GABA receptor to GABA.
- cytotoxic agent'' refers to compounds that are cytotoxic (i.e., toxic to a cell) effective for the treatment of otic disorders, e.g., autoimmune diseases of the ear and cancer of the ear, and are suitable for use in the formulations disclosed herein.
- cytotoxic small molecule refers to cytotoxic compounds that are of relatively low molecular weight, e.g., less than 1,000, or less than 600-700, or between 300-700 molecular weight, that are effective for the treatment of otic disorders, e.g.. autoimmune diseases of the ear and cancer of the ear, and are suitable for use in the formulations disclosed herein.
- Suitable "cytotoxic small molecules' * include methotrexate, cyclophosphamide, and thalidomide, as well as metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of methotrexate, cyclophosphamide, and thalidomide.
- preferred cytotoxic small molecules are the pharmaceutically active metabolites of cytotoxic agents.
- preferred metabolites are pharmaceutically active metabolites of cyclophosphamide, including but not limited to 4-hydroxycyclophosphamide, aldophosphamide, phosphoramide mustard, and combinations thereof.
- Antioxidants'' are auris-pharmaceutically acceptable antioxidants, and include, for example, b ⁇ tylated hydroxytoluene (BHT), sodium ascorbate, ascorbic acid, sodium metabismlfite and tocopherol. In certain embodiments, antioxidants enhance chemical stability where required. Antioxidants are also used to counteract the ototoxic effects of certain therapeutic agents, including agents that are used in combination with (he otic agems disclosed herein.
- BHT b ⁇ tylated hydroxytoluene
- antioxidants enhance chemical stability where required.
- Antioxidants are also used to counteract the ototoxic effects of certain therapeutic agents, including agents that are used in combination with (he otic agems disclosed herein.
- a ⁇ ris interna refers to the inner ear, including the cochlea and the vestibular labyrinth, and the round window that connects the cochlea with the middle car.
- Auris-interna bioavailability or “Amis media bioavailability” refers to the percentage of the administered dose of compounds disclosed herein that becomes available in the inner or middle ear, respectively, of the animal or human being studied.
- Auris media refers to the middle ear, including the tympanic cavity, auditory ossicles and oval window, which connects the middle ear with the inner ear.
- Blood plasma concentration refers to the concentration of compounds provided herein in the plasma component of blood of a subject.
- Auris-interna bioavailability refers to the percentage of the administered dose of compounds disclosed herein that becomes available in the inner ear of the animal or human being studied.
- Carrier materials are excipients that are compatible with the otic agenl, the auris media, the auris interna and the release profile properties of the auris-acceptable pharmaceutical formulations.
- Such carrier materials include, e.g., binders, suspending agents, disintegration agents, filling agents, surfactants, solubilizers, stabilizers, lubricants, wetting agents, diluents, and the like.
- “Auris-pharmaceutically compatible carrier materials” include, but are not limited to, acacia, gelatin, colloidal silicon dioxide, calcium glycerophosphate, calcium lactate, maltodexlri ⁇ , glycerine, magnesium silicate, polyvinylpyrrolidone (PVP), cholesterol, cholesterol esters, sodium casemate, soy lecithin, taurocholic acid, phosphatidylcholine, sodium chloride, tricalcium phosphate, dipotassium phosphate, cellulose and cellulose conjugates, sugars sodium stearoyl lactylate, carrageenan, monoglyceride, diglyceride, pregelatinized starch, and the like,
- dilute are chemical compounds that are used to dilute the otic agent prior to deliver)' and which are compatible with the auris media and/or auris interna.
- ' ⁇ Dispersing agents and/or “viscosity modulating agents” and/or “tliickening agents” are materials that control the diffusion and homogeneity of the otic agent through liquid media.
- diffusion facilitators/dispersing agents include but are not limited to hydrophilic polymers, electrolytes. Tween ® 60 or 80, PEG, polyvinylpyrrolidone (PVP; commercially known as Plasdone®), and the carbohydrate-based dispersing agents such as, for example, hydroxypropyl celluloses (e.g., KPC, HPC-SL, and HPC-L). hydroxypropyl methylcelluloscs (e.g., HPMC KlOO, HPMC K4M, HPMC K 15M, and HPMC KlOOM), earboxymethylcellulose. carboxymethylcellulose sodium, methylc ⁇ llulose, hydroxyethylcellulose, hydroxy propylcellulose,
- HPMCAS noncrystalline cellulose, magnesium aluminum silicate, triethanolamine
- polyvinyl alcohol PVA
- vinyl pyrrolidone/vinyl acetate copolymer S630
- 4-(l , 1 ,3,3-tetramethylbutyl)- phenol polymer with ethylene oxide and formaldehyde also known as tyloxapol
- poloxamers e.g., Pluronics F68®, F88®, and F108®, which are block copolymers of ethylene oxide and propylene oxide
- poloxamines e.g., Tetronic 908®, also known as Poloxamine 908®, which is a tetrafunctional block copolymer derived from sequential addition of propylene oxide and ethylene oxide to cthylenediamine (BASF Corporation, Parsippany, N.J.)
- polyvinylpyrrolidone Kl 2 polyvinylpyrrolidone Kl 7
- polyvinylpyrrohdone-'vinyl acetate copolymer S-630
- polyethylene glycol e.g., the polyethylene glycol has a molecular weight of about 300 to about 6000, or about 3350 to about 4000, or about 7000 to about 5400, sodium carboxymethylcellulose, methylcelluiose, polysorbate-80, sodium alginate, gums, such as, e.g., gum tragacanth and gum acacia, guar gum, xanthans, including xanthan gum, sugars, cellulosics, such as, e.g.. sodium carboxymethylcellulose. melhylcellulose.
- PVA polyvinyl alcohol
- Plasticizers such as cellulose or triethyl cellulo$e are also be used as dispersing agents, optional dispersing agents useful in liposomal dispersions and self-emulsifying dispersions of the otic agents disclosed herein are dimyristoyl phosphatidyl choline, natural phosphatidyl choline from eggs, natural phosphatidyl glycerol from eggs, cholesterol and isopropyl myristate.
- Drug absorption or “absorption” refers to the process of movement of the otic agent from the localized site of administration, by way of example only, the round window membrane of the inner ear, and across a barrier (the round window membranes, as described below ) into the auris interna or inner ear structures.
- co-administration or the like, as used herein, are meant to encompass administration of the otic agent to a single patient, and are intended to include treatment regimens in which the otic agents are administered by the same or different route of administration or at the same or different time.
- the terms ''effective amount” or “therapeutically effective amount,” as used herein, refer to a sufficient amount of the otic agent being administered that would be expected to relieve Io some extent one or more of the symptoms of the disease or condition being treated.
- the result of administration of the otic agents disclosed herein is reduction and/or alleviation of the signs, symptoms, or causes of AIED.
- an "effective amount” for therapeutic uses is the amount of the otic agent, including a formulation as disclosed herein required to provide a decrease or amelioration in disease symptoms without undue adverse side effects.
- therapeutically effective amount includes, for example, a prophylactically effective amount.
- An "effective amount" of a otic agent composition disclosed herein is an amount effective to achieve a desired
- an effective amount or “a therapeutically effective amount” varies, in some embodiments, from subject to subject, due to variation in metabolism of the compound
- an effective amount in. an extended-release dosing format may differ from “an effective amount” in an immediate-release dosing format based upon pharmacokinetic and pharmacodynamic considerations.
- enhancing refers to the ability to increase or prolong, either in potency or duration, the effect of odier therapeutic agents that are used in combination with the otic agents disclosed herein.
- An ''enhancing-effective amount refers to an amount of an otic agent or other therapeutic agent that is adequate to enhance the effect of another therapeutic agent or otic agent in a desired system. When used in a patient, amounts effective for this use will depend on the severity and course of the disease, disorder or condition, previous therapy, the patient's health status and response to the drugs, and the judgment of the treating physician.
- penetration enhancer refers to an agent that reduces barrier resistance (e.g., barrier resistance of the round window membrane, BLB or the like).
- the term “inhibiting” includes preventing, slowing, or reversing the development of a condition, for example, AIED. or advancement of a condition in a patient necessitating treatment. ⁇ 00901
- kit and “article of manufacture” are used as synonyms.
- the term "'modulate” includes the interaction with a target, for example, with the TNF-alpha agents disclosed herein, the activity of TNF-alpha, or other direct or indirect targets that alter the activity of TNF-alpha, including, by way of example only, to inhibit the activity of TNF-alpha, or to limit the activity of the TNF-alpha,
- Pharmacokinetics refers to the factors which determine the attainment and maintenance of the appropriate concentration of drug at the desired site within the auris media and/or auris interna.
- compositions containing ⁇ he otic agents described herein are administered to a patient susceptible to or otherwise at risk of a particular disease, disorder or condition, tor example, AIED, or patients that are suffering from diseases associated with AlED.
- diseases associated with AlED including by way of example only, Ankylosing spondylitis, Systemic Lupus Erythematosus (SLH), Sjogren's Syndrome, Cogan's disease, ulcerative colitis!.
- SSH Systemic Lupus Erythematosus
- Sjogren's Syndrome Sjogren's Syndrome
- Cogan's disease ulcerative colitis!.
- Wegener's granulomatosis inflammatory bowel disease
- rheumatoid arthritis scleroderma and Behcet's disease.
- Such an amount is defined to be a ""prophylactically effective amount or dose.” In this use, the precise amounts also depend on the patient's state of health, weight, and the lilce.
- a prodrug'- refers to the otic agent thai is converted into the parent drug in vivo.
- a prodrug is cnzymaticaliy metabolized by one or more steps or processes to the biologically, pharmaceutically or therapeutically active form of the compound.
- a pharmaceutically active compound is modified such that the active compound will be regenerated upon in vivo administration.
- the prodrug is designed to alter the metabolic stability or the transport characteristics of a drug, to mask side effects or toxicity, or to alter other characteristics or properties of a drug.
- embodiments are derivatized into suitable prodrugs.
- Solubilizers refers to auris-acceptable compounds such as triacetin, triethyleitrate, ethyl oleate, ethyl caprylate, sodium lauryl sulfate, .sodium doccusate, vitamin E TPGS, dimelhylacetainide, N-methylpyrrolidone, N-hydroxyethylpyrrolidone, polyvinylpyrrolidone, hydroxypropylmethyl cellulose, hydroxypropyl cyclodextrins, etlianol, n-butanol, isopropyl alcohol, cholesterol, bile salts, polyethylene glycol 200-600, glycofurol. transcutol®, propylene glycol, and dimethyl isosorbide and the like.
- Stabil.i7.ers refers to compounds such as any amioxidation agents, buffers, acids, preservatives and the like that are compatible with the environment of the auris media and/or amis interna.
- Stabilizers include but are not limited to agents that will do any of (1 ) improve the compatibility of excipients with a container, or a deliver ⁇ ' system, including a syringe or a glass bottle, (2) improve the stability of a component of the composition, or (3) improve formulation stability.
- Step state is when the amount of drug administered to the auris media and/or auris interna is equal to the amount of drug eliminated within one dosing interval resulting in a plateau or constant levels of drug exposure within the targeted structure.
- the term "subject” is used to mean an animal, preferably a mammal, including a human or non-human.
- the terms patient and subject are used interchangeably.
- ''Surfactants refers to compounds that are auris-acceptable, such as sodium lauryl sulfate, sodium docusate, Tween 60 or 80, triacetin, vitamin E TPGS, phospholipids, lecithins, phosphatidyl cholines (c8-cl 8), phosphatidylethanolamines (c8-cl8), phosphatidylglycerols (c8-cl8), sorbitan monooleate, poiyoxyethylene sorbitan monooleate, polysorbates, polaxomers, bile salts, glyceryl monostearate, copolymers of ethylene oxide and propylene oxide, e.g., Pluronic*' (BASF), and the like.
- BASF Pluronic*'
- surfactants include poiyoxyethylene fatty acid glycerides and vegetable oils, e.g. , poiyoxyethylene (60) hydrogenated castor oil; and poiyoxyethylene alkylethers and alkylphenyl ethers, e.g., ocloxynol 10, octoxynol 40.
- surfactants are included to enhance physical stability or for other purposes.
- treat include alleviating, abating or ameliorating a disease or condition, for example AlKD, symptoms, preventing additional symptoms, ameliorating or preventing the underlying metabolic causes of symptoms, inhibiting the disease or condition, e.g., arresting the development of the disease or condition, relieving the disease or condition, causing regression of the disease or condition, relieving a condition caused by the disease or condition, or controlling or stopping the symptoms of the disease or condition either
- the ear serves as both the sense organ that detects sound and the organ that maintains balance and body position.
- the ear is generally divided into three portions: the outer ear, middle ear and the inner ear (or auris interna).
- the outer ear is the external portion of the organ and is composed of the pinna (auricle), the auditory canal (external auditory meatus) and the outward facing portion of the tympanic membrane, also known as the ear drum.
- the pinna which is the fleshy part of the externa ear that is visible on the side of the head, collects sound waves and directs them toward the auditory canal
- the function of the outer ear in part, is to collect and direct sound waves towards the tympanic membrane and the middle ear.
- the middle ear is an air-filled cavity, called the tympanic cavity, behind the tympanic membrane.
- the tympanic membrane also known as the ear drum, is a thin membrane that separates the externa) ear from the middle ear.
- the middle ear lies within the temporal bone, and includes within this space the three ear bones (auditory ossicles): the malleus, the incus and the stapes.
- the auditor)' ossicles are linked together via tiny ligaments, which form a bridge across the space of the tympanic cavity.
- the malleus which is attached to the tympanic membrane at one end, is linked to the incus at its anterior end, which in turn is linked to the stapes.
- the stapes is attached to the oval window, one of two windows located winthin the tympanic cavity.
- a fibrous tissue layer known as the annular ligament connects the stapes to the oval window.
- the auditory ossicles are arranged to provide a mechanical linkage between the tympanic membrane and the oval window of the fluid-filled auris interna, where sound is transformed and transduced to the auris interna for further processing.
- Stiffness, rigidity or loss of movement of the auditory ossicles, tympanic membrane or oval window leads to hearing loss, e.g. otosclerosis, or rigidity of the stapes bone.
- the tympanic cavity also connects to the throat via the eustachian tube.
- the eustachian tube provides the ability to equalize the pressure between the outside air and the middle ear cavity.
- the round window a component of the auris interna but which is also accessible within the tympanic cavity, opens into the cochlea of the auris interna.
- the round window is covered by a membrane, which consists of three layers; an external or mucous layeiv an intermediate or fibrous layer, and an internal membrane, which communicates directly with the cochlear fluid.
- the round window therefore, has direct communication with the auris interna via the internal membrane.
- Movements in the oval and round window are interconnected, i.e. as the stapes bone transmits movement from the tympanic membrane to the oval window to move inward against the auris interna fluid, the round window is correspondingly pushed out and away from the cochlear fluid.
- This movement of the round window allows movement of fluid within the cochlea, which eventually leads in turn to movement of the cochlear inner hair cells, allowing hearing signals to be transduced.
- Stiffness and rigidity in the round window leads to hearing loss because of the lack of ability of movement in the cochlear fluid.
- Recent studies have focused on implanting mechanical transducers onto the round window, which bypasses the normal conductive pathway through the oval window and provides amplified input into the cochlear chamber.
- Auditory signal transduction takes place in the auris interna.
- the fluid-filled inner ear, or auris interna consists of two major components: the cochlear and the vestibular apparatus.
- the cochlea is the portion of the auris interna related to hearing.
- the cochlea is a tapered tube-like structure which is coiled into a shape resembling a snail.
- the inside of the cochlea is divided into three regions, which is further defined by the position of the vestibular membrane and the basilar membrane.
- the portion above the vestibular membrane is the scala vestibuli, which extends from the oval window to the apex of the cochlea and contains perilymph fluid, an aqueous liquid low in potassium and high in sodium content.
- the basilar membrane defines the scala tympani region, which extends from the apex of the cochlea to the round window and also contains perilymph.
- the basilar membrane contains thousands of stiff fibers, which gradually increase in length from the round window to the apex of the cochlea.
- the fibers of the basement membrane vibrate when activated by sound.
- Tn between the scala vestibuli and the scala tympani is the cochlear duct, which ends as a closed sac at the apex of the cochlea.
- the cochlear duct contains endolymph fluid, which is similar to cerebrospinal fluid and is high in potassium.
- the Organ of Corti the sensory organ for hearing, is located on the basilar membrane and extends upward into the cochlear duct.
- the Organ of Corti contains liair cells, which have hairlike projections that extend from their free surface, and contacts a gelatinous surface called the tectorial membrane. Although hair cells have no axons, they are surrounded by sensory nerve fibers that form the cochlear branch of the vestibulocochlear nerve (cranial nerve VIO).
- the oval window also known as the elliptical window communicates with the stapes to relay sound waves that vibrate from the tympanic membrane. Vibrations transferred to the oval window increases pressure inside the fluid-filled cocljea via the perilymph and scala vestibuli/scala tympani, which in turn causes the membrane on the round window to expand in response.
- the concerted inward pressing of the oval window/outward expansion of the round window allows for the movement of fluid within the cochlea without a change of intra-cochlear pressure.
- vibrations travel through the perilymph in the scala veslibuli, they create corresponding oscillations in the vestibular membrane.
- the auris interna is located in part within the osseous or bony labyrinth, an intricate series of passages in the temporal bone of the skull.
- the vestibular apparatus is the organ of balance and consists of the three semi-circular canals and the vestibule.
- the three semi-circular canals are arranged relative to each other such that movement of the head along the three orthogonal planes in space can be detected by the movement of the fluid and subsequent signal processing by the sensory organs of the semi-circular canals, called the crista amuplkris.
- the crista ampullaris contains hair cells and supporting cells, and is covered by a dome-shaped gelatinous mass called the cupula.
- the hairs of the hair cells are embedded in ihe cupula.
- the semi-circular canals detect dynamic equilibrium, the equilibrium of rotational or angular movements.
- the vestibule is the central portion of the auris interna and contains mechanoreceptors bearing hair ceils that ascertain static equilibrium, or the position of the head relative to gravity. Static equilibrium plays a role when the head is motionless or moving in a straight line.
- the membranous labyrinth in the vestibule is divided into two sac-like structures, the utricle and the saccule. Each structure in turn contains a small structure called a macula, which is responsible for maintenance of static equilibrium.
- the macula consists of sensory hair cells, which are embedded in a gelatinous mass (similar to the cupula) that covers the macula. Grains of calcium carbonate, called otoliths, are embedded on the surface of the gelatinous layer.
- the hairs are straight along the macula.
- the gelatinous mass and otoliths tilts correspondingly, bending some of the hairs on the hair cells of the macula. This bending action initiates a signal impulse to the central nervous system, which travels via the vestibular branch of the vestibulocochlear nerve, which in turn relays motor impulses to the appropriate muscles to maintain balance.
- the drug formulation will first be placed in the middle or inner ear, including the cochlea and vestibular labyrinth: one option is to use a syringe/needle or pump and inject the formulation across the tympanic membrane (the eardrum). For cochlear and vestibular labyrinth delivery, one option is to deliver the active ingredient across the round window membrane or even by
- Rodent animal models for inner ear disease e.g., inner ear disease models in. guinea pigs
- the middle ear of the guinea pig (or bulla) is a cavity that contains all of the cochlea; the cochlea is anchored to the bulla via the basal turn, its apex residing in the cavity.
- the human cochlea is imbedded into the temporal bone and the only access to the human cochlea is through the round window.
- studies in guinea pigs that overfill the bulla and'or inject formulations towards the anterior quadrant of the tympani, or more generally away from the round window niche will result in high perilymph exposure because of drug diffusion through the cochlea apex.
- This situation is not possible in humans because the human cochlea is imbedded into the temporal bone and as such the only access to the cochlea is on and/or through the round window or the elliptical/oval window.
- the ossicle chains in guinea pigs are adjacent to the round window.
- the location of the ossicle chains next to the round window in guinea pig ears adversely affects the ABR threshold in experiments with guinea pigs.
- the human ear is anatomically different from rodent ears; the ossicle chains and/or stapes are anatomically located away from the round window. Jn certain instances, an auris formulation injected intratympanically into a human ear does not make contact with the stapes and does not adversely affect the ABR threshold.
- the reliability of animal models of inner ear diseases as a predictor of efficacy in human clinical trials is limited by the anatomical difference between the human car and animal cars.
- a guinea pig animal model for inner ear disease utilizes an injection via a hole drilled into the bulla, i.e., the cavity surrounding the cochlear bones.
- the bulla procedure leads to a local inflammatory reaction and a rapid accumulation of fluids within the bulla cavity, a condition that lasts for several days.
- an accumulation of significant volumes of fluids in the bulla (about a 1/3-1/2 of the total bulla volume) seen with the bulla injection rapidly erodes any auris formulation injected, primarily by diluting the formulation and reverting a formulation (e.g., a gel formulation) to a liquid that drains away via the eustachian tube.
- a formulation e.g., a gel formulation
- a gel formulation comprising a poloxamer will not form a gel at concentration below 12- 14%, and at concentrations less than 35% coxicentration will gel at temperatures higher than 37 °C.
- a guinea pig model is of limited utility for testing the efficacy of an auris formulation for administration to humans due the accelerated clearance of the gel from the bxiiia compartment of a guinea pig.
- a 17% Pluronic F-127 gel injection is cleared from the bulla of a guinea pig in less than 2 days.
- a guinea pig animal model for inner ear disease utilizes an injection through the tympanic membrane.
- an intratympanic injection is not associated with fluid accumulation at any of the time points evaluated (up toIO days), hi some instances, injection of an auris formulation described herein (e.g. a gel formulation) via the tympanic route allows for detectable amounts of the formulation (e.g., a gel) in the inner ear of a guinea pig up to at least 5 days.
- animal models e.g., guinea pig models for inner ear diseases
- intratympanic injections are limited by the volume that can be injected through the tympanic route.
- the round window niche and membrane are located just opposite the tympanic membrane in the posterior superior quadrant, in certain instances, about 50 mL can be injected within this quadrant in a 250-350g guinea pig.
- a larger volume up to 70 mL
- most of the gel migrates towards the round window.
- larger volumes (100-120mci) are injected in the anterior quadrant, but this action fills the bulla cavity and promotes drug transfer across the apical part of the cochlea (due to the bone structure thinness of the cochlea in rodents).
- injection of larger volumes in any of these quadrants leads to tympanic perforation and presence of the gel in the external ear canal.
- the volume injected has an impact on the hearing threshold (measured by ABR).
- intratyrapanic injections volumes up to 50 mL do not produce any shift in hearing threshold; but volumes of 90 and 120 mL produce an ABR threshold shift within 1 day,
- the anatomical difference between human and animal ears and the variability in experiemental outcomes lends a low predictive value to animal testing data for use in subsequent human clinical trials.
- the invasive procedures used in animal models of inner ear disease are not applicable in a clinical setting.
- otic formulations that comprise a dye (e.g., a Trypan blue dye, Evans blue dye) or other tracer compound.
- a dye e.g., a Trypan blue dye, Evans blue dye
- addition of an auris-compalible dye to an otic formulation described herein aids visualization of any administered formulation in a ear (e.g., a rodent ear and/or a human ear).
- an otic composition comprising a dye or other tracer compound eliminates the need for invasive procedures that are currently used in animal models to monitor the concentrations of drugs in the endolymph and/or perilymph.
- intratympanic injections require the need of a specialist and the formulation needs to be delivered to a specific site of the ear to maximize efficiency of the medication delivered.
- a visualization technique for any formulation described herein allows for visualization of a dosing site (e.g., the round window) so thai the medication is applied in the proper place.
- a fomulation comprising a dye allows visualization of the formulation during administration of the formulation to an ear (e.g., a human ear), ensures that the medication will be delivered at the intended site, and avoids any complications due to incorrect placement of a formulation.
- dyes that are compatible with the otic compositions described herein include Evans blue (e.g., 0.5% of the total weight of an otic formulation), Methylene blue (e.g., 1% of the total weight of an otic formulation), Isosulfan blue (e.g., I % of the total weight of an otic formulation), Trypan blue (e.g., 0.15% of the total weight of an otic formulation), and/or indocyanine green (e.g., 25mg/vial).
- FD&C red 40 FD&C red 3, FD&C yellow 5, FD&C yellow 6, FD&C blue 1 , FD&C bluc2, FD&C green 3
- fluorescence dyes e.g., Fluorescein isothiocyanate, rhodamine, Alexa Fluors, DyLight Fluors
- an&'or dyes that are visualizable in conjunction with non-invasive imaging techniques such as MRI, CAT scans, PET scans or the like (e.g., Gadolinium-based MRI dyes, iodine-base dyes, barium-based dyes or the like) are also contemplated for use with any otic fomulation described herein.
- concentration of a dye in any otic formulation described herein is less than 2%, less than 1.5%, less than 1%, less than 0.5%, less than 0.25%. less than 0.1 %, or less than 100 ppm of the total weight and/or volume of any formulation described herein.
- auris-compatible formulations that comprise a dye
- the ability to visualize a controlled release otic formulation comprising a dye in an ear meets a long standing need for suitable testing methods that are applicable to the development of intratympanic otic compositions suitable for human use.
- the ability to visxialize a controlled release otic formulation comprising a dye allows for testing of any otic formulation described herein in human clinical trials.
- formulations described herein are suitable for the treatment and/or prevention of diseases or conditions associated with the middle and inner ear, including the cochlea, including vertigo, tinnitus, hearing loss, otosclerosis, balance disorders, and Meniere's disease (endolymphatic hydrops).
- otic disorders e.g., amis interna disorders
- nystagmus e.g., vertigo
- tinnitus e.g., tinnitus
- inflammation e.g., swelling, infection and congestion.
- Meniere's Disease is an idiopathic condition dutraclerized by sudden attacks of vertigo, nausea and vomiting that may last for 3 to 24 hours, and may subside gradually. Progressive hearing loss, tinnitus and a sensation of pressure in the ears accompanies the disease through time.
- the cause of Meniere's disease is likely related to art imbalance of auris interna fluid homeostasis, including an increase in production or a decrease in resorption of auris interna fluid.
- the cause of symptoms associated with Meniere's disease is likely an imbalance of inner ear fluid homeostasis, including an increase in production or a decrease in reabsorption of inner ear fluid.
- controlled release formulations disclosed herein comprising antiviral agents, e.g., gancielvir, acyclovir, fatnovir, and valgancyclovir, is administered to the ear for localized treatment of Meniere's disease.
- antiviral agents e.g., gancielvir, acyclovir, fatnovir, and valgancyclovir
- VP antagonists including infusion of OPC-31260 (a competitive antagonist of V r R) into the scala tympani resulted in a marked reduction of Meniere's disease symptoms.
- OPC-31260 a competitive antagonist of V r R
- Other VP antagonists include WAY-140288, CL-385004, tolvaptan, conivaptan, SR 121463A and VPA 985.
- Surgical procedures have also been used to relieve symptoms of Meniere's disease, including destruction of vestibular function to relieve vertigo symptoms. These procedures aim to either reduce fluid pressure in the inner ear and/or to destroy inner ear balance function.
- An endolymphatic shunt procedure which relieves fluid pressure, are placed in the inner ear to relieve symptoms of vestibular dysfunction. Severing of the vestibular nerve may also be employed, which may control vertigo while preserving hearing.
- Another approach to destruction of vestibular function for the treatment of severe Meniere's disease is intratympanic application of an agent that destroys sensory hair cell function in the vestibular system, thereby eradicating inner ear balance function.
- Various antimicrobial agents are used in the procedure, including aminoglycosides such as gentamicin and streptomycin. The agents are injected through the tympanic membrane using a small needle, a tympanostomy tube with or without a wick, or surgical catheters.
- Various dosing regimens are used to administer the antimicrobial agents, including a low dose method in which less of the agents are administered over longer periods of time (e.g., one month between injections), and high dose methods in which more of the agents are administered over a shorter time frame (e.g., every week).
- a low dose method in which less of the agents are administered over longer periods of time (e.g., one month between injections)
- high dose methods in which more of the agents are administered over a shorter time frame (e.g., every week).
- the high dose method is typically more effective, it is more risky, as it may result in hearing loss.
- formulations disclosed herein are also useful for administration of antimicrobial agents, e.g., gentamicin and streptomycin, for disabling the vestibular apparatus to treat Meniere's disease.
- antimicrobial agents e.g., gentamicin and streptomycin
- the formulations disclosed herein are used to maintain a steady release of the active agents inside the tympanic membrane, thereby avoiding the need for multiple injections or the insertion of a tympanostomy tube.
- the formulations disclosed herein can also be used to administer higher doses of the antimicrobial agents with a decreased risk of hearing loss.
- Meniere's Syndrome which displays similar symptoms as Meniere's disease, is attributed as a secondary affliction to another disease process, e.g. thyroid disease or auris interna
- Meniere's syndrome thus, are secondary effects to various process that interfere with normal production or resportption of endolymph, including endocrine abnormalities, electrolyte imbalance, autoimmune dysfuntio ⁇ , medications, infections (e.g. parasitic infectious) or hyperlipider ⁇ ia. Treatment of patients afflicted with Meniere's Syndrome is similar to Meniere's Disease.
- Sensorineural hearing loss is a type of hearing loss which results from defects (congenital and acquired) in the vestibulocochlear nerve (also known as cranial nerve VlU), or sensory cells of the inner ear. The majority of defects of the inner ear arc defects of otic hair cells.
- Aplasia of the cochlea, chromosomal defects, and congenital cholesteatoma are examples of congenital defects which can result in sensorineural hearing loss.
- inflammatory diseases e.g. suppurative labyrinthitis, meningitis, mumps, measles, viral syphilis, and autoimmune disorders
- Meniere's Disease exposure to ototoxic drugs (e.g. aminoglycosides, loop diuretics, antimetabolites, salicylates, and cisplatin), physical trauma, presbyacusis, and acoustic trauma (prolonged exposure to sound in excess of 90 dB) can all result in acquired sensorineural hearing loss.
- the sensorineural hearing loss is called central healing loss. If the defect resulting in sensorineural hearing loss is a defect in the auditory pathways, the sensorineural hearing loss is called cortical deafness.
- sensorineural hearing loss occurs when the components of the auris interna or accompanying neural components are affected, and may contain a neural, i.e. when the auditory nerve or auditory nerve pathways in the brain are affected, or sensory component.
- Sensory- hearing loss are hereditary, ⁇ r it are caused by acoustic trauma (i.e. very loud noises), a viral infection, drug-induced or Meniere's disease.
- Neural hearing loss may occur as a result of brain tumors, infections, or various brain and nerve disorders, such as stroke.
- Some hereditary diseases, such as Refsum's disease (defective accumulation of branched fatty acids) may also cause neural disorders affecting hearing loss.
- Auditory nerve pathways are damaged by demyelinating diseases, e.g. idiopathic inflammatory demyelinating disease (including multiple sclerosis), transverse myelitis, Devic's disease, progressive multifocal leukoencephalopathy, Guillain-Barre syndrome, chronic inflammatory demyelinating polyneuropathy and anti-MAG peripheral neuropathy.
- demyelinating diseases e.g. idiopathic inflammatory demyelinating disease (including multiple sclerosis), transverse myelitis, Devic's disease, progressive multifocal leukoencephalopathy, Guillain-Barre syndrome, chronic inflammatory demyelinating polyneuropathy and anti-MAG peripheral neuropathy.
- demyelinating diseases e.g. idiopathic inflammatory demyelinating disease (including multiple sclerosis), transverse myelitis, Devic's disease, progressive multifocal leukoencephalopathy, Guillain-Barre syndrome, chronic inflammatory demyelinating polyn
- the incidence of sudden deafness, or sensorineural hearing loss occurs in about 1 in 5000 individuals, and are caused by viral or bacterial infections, e.g. mumps, measles, influenza, chickenpox, cytomegalovirus, syphillis or infectious mononucleosis, or physical injury to the inner ear organ. In some cases, no cause can be identified. Tinnitus and vertigo may accompany sudden deafness, which subsides gradually. Oral corticosteroids are frequently prescribed to treat sensorineural hearing loss. In some cases, surgical intervention are necessary. Other treatments include AM-IOl and AM-111, compounds under development for the treatment of auris interna tinnitus and acute sensorineural hearing loss. (Auris Medical AG, Basel, Switzerland).
- Noise induced hearing loss is caused upon exposure to sounds that are too loud or loud sounds that last a long time. Hearing ioss may occur from prolonged exposure to loud noises, such as loud music, heavy equipment or machinery, airplanes or gunfire. Long or repeated or impulse exposure to sounds at or above 85 decibels can cause hearing loss.
- NIIlL causes damage to the hair cells and/or the auditory nerve. The hair ceils are small sensory cells that convert sound energy into electrical signals that travel to the brain. Impulse sound can result in immediate hearing ioss that are permarjent.
- This kind of hearing loss are accompanied by tinnitus— a ringing, buzzing, or roaring in the ears or head- -WhJCh may subside over time.
- Hearing loss and tinnitus are experienced in one or both ears, and tinnitus may continue constantly or occasionally throughout a lifetime. Permanent damage to hearing loss is often diagnosed. Continuous exposure to loud noise also damages the structure of hair cells, resulting in hearing loss and tinnitus, although the process occurs more gradually than for impulse noise.
- an otoprotectant can reverse, reduce or ameliorate NTRL.
- otoprotectanls that treat or prevent N1HL include, but are not limited to, ⁇ -melhionine, L- methionme, ethionine.
- IGF-I insulin-like growth factor 1
- antioxidant therapy including treatment with alpha lipoic acid.
- Tinnitus is defined as the perception of sound in the absence of any external stimuli. It may occur in one or both ears, continuously or sporadically, and is most often described as a ringing sound. It is most often used as a diagnostic symptom for other diseases. There are two types of tinnitus: objective and subjective. The former is a sound created in the body which is audible to anyone. The latter is audible only to the affected individual. Studies estimate that over 50 million Americans experience some form of tinnitus. Of those 50 million, about 12 million experience severe tinnitus.
- tinnitus results from damage to otic structures (e.g. stereocillia), the dysfunction of one or more molecular receptors, and/or the dysfunction of one or more neural pathways.
- tinnitus results from excitotoxicity caused by abnormal activity of an NMDA receptor.
- tinnitus results from by dysfunction of an ⁇ 9 and/or ⁇ lO acetylcholine receptor.
- tinnitus results from damage to the vestibulocochlear nerve.
- a reduction in neurotransmitter reuptake treats, and/or ameliorates the symptoms of tinnitus.
- antagonism of an NK 1 receptor treats, and/or ameliorates the symptoms of tinnitus.
- a reduction in neurotransmitter reuptake and antagonism of an NKl receptor beats, and/or ameliorates the symptoms of tinnitus.
- Lidocaine administered by IV, reduces or eliminates the noise associated with tinnitus in about 60-80% of sufferers.
- Selective neurotransmitter reuptake inhibitors such as nortriptyline, sertraline, and paroxetine, have also demonstrated efficacy against tinnitus.
- Benzodiazepines are also prescribed to treat tinnitus.
- AIED Autoimmune inner ear disease
- AIED occurs without systemic autoimmune symptoms, but up to orte-third of patients also suffer from a systemic autoimmune illness, such as inflammatory bowel disease, rheumatoid arthritis, Ankylosing spondylitis, Systemic Lupus Erythematosus (SLE), Sjogren's Syndrome, Cogan's disease, ulcerative colitis, Wegener's granulomatosis and
- a systemic autoimmune illness such as inflammatory bowel disease, rheumatoid arthritis, Ankylosing spondylitis, Systemic Lupus Erythematosus (SLE), Sjogren's Syndrome, Cogan's disease, ulcerative colitis, Wegener's granulomatosis and
- Behcet's disease a multisystem disease, also commonly has audiovestibular problems. There is some evidence for food-related allergies as a cause for cochlear and vestibular
- the immune system normally performs a cruical role in protecting the auris interna from invasive pathogens such as bacteria and viruses.
- AIED the immune system itself begins to damage the delicate auris interna tissues.
- the auris interna is fully capable of mounting a localized immune response to foreign antigens. (Harris. Otolaryngol. Head Neck Surg. (1983) 91. 18-32).
- a foreign antigen enters the auris interna, it is first processed by immunocompetent cells which reside in and around the endolymphatic sac. Once the foreign antigen has been processed by these immunocompetent cells, these cells secrete various cytokines which modulate the immune response of the auris interna.
- IL-I lnterleukin 1
- IL-2 secretion results in differentiation of pluripotet T-cells into helper, cytotoxic and suppressor T-cell subtypes. IL-2 also assists T helper cells in the activation of B lymphocytes and probably plays a pivotal role in ihe immunoregulation of the immune response of the auris interna. IL-2 has been identified within the perilymph of the auris interna as early as 6 h after antigen challenge with peak levels at 18 h after antigen chalenge. The perilymphatic levels of IL-2 then dissipate, and it is no longer present within the perilymph at 120 hours post antigen challenge (Gloddek, Acta Otolaryngol. (1989) 108, 68-75).
- l00148jBoth IL-I (5 and tumor necrosis factor- ⁇ (TN F- ⁇ ) may play a key role in the initiation and amplification of the immune response.
- JL-I ⁇ is expressed by the fibrocytes of the spiral ligament in the presence of trauma such as surgical trauma or acoustic trauma in a nonspecific response.
- THF- ⁇ is expressed either by infiltrating systemic cells or by resident cells contained within the endolymphatic sac in the presence of antigen. THF- ⁇ is released as part of the adaptive (specific) immune response in animal models.
- antigen is injected into the auris internas of mice, IL-I ⁇ and TNP-(X are both expressed and a vigouous immune response occurs.
- agents which downregulate or block the specific immune response, and in particular the effect of TNF- ⁇ . might be able to prevent the excessive immune response seen when both the specific and nonspecific immune responses are simultaneously activated (Satoh, Laryngoscope (2002). 112, 1627-1634).
- Treatment of autoimmune ear disease may consist of anti-TNF agents.
- Trials using etanercept (ENBREl/) an anti-TNF drug is emerging as a promising agent for treatment of autoimmune inner ear disease.
- etanercept ENBREl/
- an anti-TNF drug is emerging as a promising agent for treatment of autoimmune inner ear disease.
- REMlCADE* adaltmumab
- HL 1 MlRA* adaltmumab
- Trial protocols include injections of anti-TNF agents as an injection on a twice- weekly basis.
- steroids have been used, e.g. prednisone or decadron, have also been tried with some success.
- Chemotherapeutic agents e.g. Cytoxan, azathiaprine or methotrexate are used on a long-term basis to treat autoimmune inner ear disorders.
- Plasmapheresis procedures have also been tried with some success. (Luetje et al. Am. J.
- controlled release antimicrobial agent compositions aod formulations disclosed herein are administered for the treatment of AIED.
- formulations disclosed herein comprising antiviral agents are administered for treatment of AIED.
- the antimicrobial agent formulations disclosed herein are administered for the treatment of AJED in conjunction with other pharmaceutical agents useM for treating the same conditions or symptoms of the same conditions, including steroids, cytotoxic agents, collagen, gamma globulin infusion, or other immune modulating drugs.
- Steroids include, e.g., prednisone or decadron.
- Cytotoxic agents for the treatment of AJED include, e.g., methotrexate, cyclophosphamide, and thalidomide. Plasmapheresis procedures are optionally used. Treatment with oral collagen, gamma globulin infusions, or other immune modulating drugs (e.g. beta-interferon, alpha-interferon or Copaxone) is also optionally used in combination with the antimicrobial agent formulations disclosed herein.
- the additional pharmaceutical agents are optionally administered together with the controlled release formulations disclosed herein, or through other modes of administration, e.g., orally, by injection, topically, nasally or through any other suitable means.
- the additional pharmaceutical agents are optionally co-adininistered, or administered at different time periods.
- Auditory nerve tumors including acoustic neuroma, acoustic neurinoma, vestibular schwannoma and eighth nerve tumor
- Auditory nerve rumors account for approximately 7-8% of all tumors originating in the skull, and are often associated with the diagnosis of neurofibromatosis in a patient.
- some symptoms include hearing loss, tinnitus, dizziness and loss of balance.
- Other more serious symptoms may develop as (he tumor becomes larger, which may compress against the facial or trigemmmal nerve, which may affect connections between the brain and the mouth, eye or jaw.
- Smaller tumors are removed by microsurgery, or sterotactic radiosurgical techniques, including fractionated ste ⁇ ttactic radiotherapy.
- Malignant Schwannomas are treated with chemotherapeutic agents, including vincristine, adriamycin, cyclophosphamide and imidazole carboxamide.
- Benign paroxysmal positional vertigo is caused by the movement of free floating calcium carbonate crystals (otoliths) from the utricle to one of the semicircular canals, most often the posterior semicircular canal. Movement of the head results in the movement of the otoliths causing abnormal endolymph displacement and a resultant sensation of vertigo. The episodes of vertigo usually last for about a minute and are rarely accompanied by other auditory symptoms.
- otoliths free floating calcium carbonate crystals
- cancer of the ear is often associated with long-term and untreated otitis, suggesting a link between clironic inflammation and development of the cancer, at least in some cases.
- Tumors in the ear can be benign or malignant, and they can exist in the external, middle, or inner ear.
- Symptoms of ear cancer include otorrhea, otalgia, hearing loss, facial palsy, tinnitus, and vertigo. Treatment options are limited, and include surgery, radiotherapy,
- additional pharmaceutical agents are used to treat symptoms or conditions associated with the cancer, including corticosteroids in the ease of facial palsy, and antimicrobial agents when otitis is present.
- cytotoxic agents e.g., methotrexate, cyclophosphamide, and thalidomide
- cytotoxic agents for the treatment of cancer of the ear include anemia, neutropenia, bruising, nausea, dermatitis, hepatitis, pulmonary fibrosis, teratogenicity, peripheral neuropathy, fatigue, constipation.
- the cytotoxic agents are methotrexate (RHEUMATREX®, Amethopterin) cyclophosphamide (CYTOXAN®), and thalidomide (TH ALIDOM ED®), All of the compounds can be used to treat cancer, including cancer of the ear. Further, all of the compounds have anti-inflammatory properties and can be used in the formulations and compositions disclosed herein for the treatment of inflammatory disorders of the ear, including AIED.
- cytotoxic agents are not without the potential for serious adverse side effects. Moreover, cytotoxic agents which demonstrate efficacy but are otherwise not approvable because of safety considerations is also contemplated within the embodiments disclosed herein.
- cytotoxic agents to the target otic structures for treatment of autoimmune and/or inflammatory disorders, as well as cancer of the ear, will result in the reduction or elimination of adverse side effects experienced with systemic treatment.
- localized treatment with the cytotoxic agents contemplated herein will also reduce the amount of agent needed for effective treatment of the targeted disorder due. for example, to increased retention of the active agents in the auris interna and/or media, to the existence of the biological blood barrier in the auris interna, or to the lack of sufficient systemic access to the auris media.
- cytotoxic agents used in the compositions, formulations, and methods disclosed herein are metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of cytotoxic agents, including methotrexate, cyclophosphamide, and thalidomide.
- Particularly preferred are metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of cytotoxic agents, e.g., methotrexate, cyclophosphamide, and thalidomide, that retain at least partially the cytotoxicity and anti-inflammatory properties of the parent compounds.
- analogues of thalidomide used in the formulations and compositions disclosed herein are ienalidomide
- Cyclophosphamide is a prodrug that undergoes in vivo metabolism when administered systemically.
- the oxidized metabolite 4-hydroxycyciophosphamide exists in equilibrium with aldophosphamide, and the two compounds serve as the transport forms of the active agent phosphoramide mustard and the degradation byproduct acrolein.
- preferred cyclophosphamide metabolites for incorporation into the formulations and compositions disclosed herein are 4-hydroxycyclophosphamide, aldophosphamide, phosphoramide mustard, and combinations thereof.
- cytotoxic agents used in the compositions, formulations, and methods disclosed herein, particularly for the treatment of cancer of the ear are any conventional cher ⁇ otherpeutic agents, including acridine carboxamide, actinoniycin, 17-N-allylairtino-17-demethoxygeldanamycin, aminopterin, amsacrine, anthracycline, antineoplastic, antineoplaston, 5-azacytidinc, azathioprine, BL22, bendamustine, biricodar. bleomycin, bortezomib, bryostatin, busulfan, calyculin.
- acridine carboxamide including acridine carboxamide, actinoniycin, 17-N-allylairtino-17-demethoxygeldanamycin, aminopterin, amsacrine, anthracycline, antineoplastic, antineoplaston, 5-azacytidinc,
- camptothecin capecitabine, carboplatin, chlorambucil, cisplatin, cladribine, clofarabine, cytarabine, dacarbazine, dasatinib, daunombicin, decitabine, dichloroacetic acid, discodermolide, docetaxel, doxorubicin, epirubiein, epothilone, eribulin, estramustine, etoposide, exatecan, exisulind, ferrugiiiol, f ⁇ oxuridine, fludarabine.
- fluorouracil fosfestrol, fbtemustine, gemcitabine, hydroxyurea, IT-101, idarubicin, ifosfamide, imiquimod, irinotecan, irofulven, ixabepilone.
- laniquidar lapatinib, Ienalidomide, lomustine, lurtoteean, mafosfamide, masoprocol, mechlorethamine, melphalan, mereaptopurine, mitomycin, mitotane, mitoxantrone.
- PAC-I paclitaxel.
- pemetrexed pemetrexed, pentostatin, pipobroman, pixantrone, plicamycin, procarbazine, proteasome inhibitors (e.g., bortezomib), raltitrexed, rebeccamycin, rubitecan, SN-38,
- salinosporamide A satrapiatin, streptozotocin. swainsomne, tariquidar, taxane, tegalur-uracil, temo ⁇ olomide, testolactone, thioTEPA, tioguanine, topotecan, trabectedin, tretinoin, triplatin tetraxiitrale, t ⁇ is(2-chloroelhyl)araine, troxacitabine, uracil mustard, valrubicin. vinblastine, vincristine, vinorelbine, vorinostat. and zosuquidar.
- a cholesteatoma is a hyperprolif -eralive cyst often found in the middle ear. Cholesteatoma are classified as congenital or acquired. Acquired cholesteatomas result from retraction of the ear drum (primary) and/or a tear in the ear drum (secondary).
- Complications associated with a growing cholesteatoma include injury to the osteoclasts and, in some cases, deter ioration of the thin bone layer separating the top of the ear from the brain.
- Damage to the osteoclasts results from the persistent application of pressure to the bones resulting from the expansion of the cholesteatoma. Additionally, the presence of multiple cytokines (e.g.
- TNF- ⁇ , TGF- ⁇ l , TGF- ⁇ 2, XI-I , and IL-6) in the epithelium of the cholesteatoma can result in further degradation of the surrounding bones.
- ⁇ 00166 ⁇ Patients with a cholesteatoma often present with earache, hearing loss, mucopurulent discharge, and/or dizziness. Physical examination can confirm the presence of a cholesteatoma.
- Symptoms which can be identified upon physical examination include damage to the ossicles, and a canal filled with mucopus and granulation tissue.
- ethacrynic acid and furosemide ethacrynic acid and furosemide
- aspirin ethacrynic acid and furosemide
- aspirin-like substances e.g. salicylates
- quinine e.g. quinine
- Deterioration of the auris interna organ are hastened by impaired kidney function, which results in decreased clearance of the affecting drugs and their metabolites.
- the drugs may affect both hearing and equilibrium, but likely affects hearing to a greater extent.
- neomycin, kanamycin, amikacin have a greater effect on hearing than on balance.
- the antibiotics vioraycin, gentamicin and tobramycin affect both hearing and eq ⁇ ilibirum.
- Streptomycin another commonly administered antibiotic, induces vertigo more than loss of hearing, and can lead to Dandy's syndrome, where walking in the dark becomes difficult and induces a sensation of the environment moving with each step.
- Aspirin when taken in very high doses, may also lead Io temporary hearing loss and tinnitus, a condition where sound is perceived in the absence of external sound.
- quinine, ethacryinic acid and f ⁇ rosemide can result ⁇ a temporary or permanent hearing loss.
- Excitotoxicity refers to the death or damaging of neurons and/or otic hair cells by glutamate and/or similar substances.
- Glutamate is the most abundant excitatory neurotransmitter in the central nervous system. Pre-synaptic neurons release glutamate upon stimulation, it flows across the synapse, binds to receptors located on post-synaptic neurons, and activates these neurons.
- the glutamate receptors include the NMDA, AMPA, and kainate receptors.
- Glutamate transporters are tasked with removing extracellular glutamate from the synapse. Certain events (e.g. ischemia or stroke) can damage the transporters. This results in excess glutamate accumulating in the synapse. Excess glutamate in synapses results in the over-activation of the glutamate receptors.
- the AMPA receptor is activated by the binding of both giutamate and AMPA. Activation of certain isoforms of the AMPA receptor results in the opening of ton channels located in the plasma membrane of the neuron. When the channels open, Na + and Ca * ' ions flow into the neuron and K ' ions flow out of the neuron.
- the NMDA receptor is activated by the binding of both glutamate and NMDA. Activation of the NMDA receptor, results in the opening of ion channels located in the plasma membrane of the neuron. However, these channels are blocked by Mg 2+ ions. Activation of the AMPA receptor results in the expulsion of Mg 2 ⁇ ions from the ion channels into the synapse. When the ion channels open, and the Mg 21 ions evacuate the ion channels, Na * and Ca 2+ ions flow into the neuron, and K + ions flow out of the neuron.
- TMs allows abnormally high levels of Ca 2 ' and Na ⁇ to enter the neuron.
- the influx of these levels of Ca 2- and Na ' into the neuron causes the neuron to fire more often, resulting in a rapid buildup of free radicals and inflammatory compounds within the cell.
- the free radicals eventually damage the mitochondria, depleting the cell's energy' stores.
- excess levels of Ca 2- and Na * ions activate excess levels of enzymes including, but not limited to, phospholipases, endomicleases, and proteases.
- enzymes including, but not limited to, phospholipases, endomicleases, and proteases.
- the over-activation of these enzymes results in damage to the cytoskeleton, plasma membrane, mitochondria, and DNA of the sensory neuron.
- Endolymphatic hydrops refers to an increase in the hydraulic pressure within the endolymphatic system of the inner ear.
- the endolyraph and perilymph are separated by thin membranes which contain multiple nerves. Fluctuation in the pressure stresses the membranes and the nerves they house. If the pressure is great enough, disruptions may form in the membranes. This results in a mixing of the fluids which can lead to a depolarization blockade and transient loss of function. Changes in the rate of vestibular nerve firing often lead to vertigo. Further, the Organ of Corti may also be affected. Distortions of the basilar membrane and the inner and outer hair cells can lead to hearing loss and'or tinnitus.
- ⁇ 001761 causes include metabolic disturbances, hormonal imbalances, autoimmune disease, and viral, bacterial, or fungal infections. Symptoms include hearing loss, vertigo, tinnitus, and aural fullness. Nystagmus may also be present. Treatment includes systemic administration of benzodiazepine, diuretics (to decrease the fluid pressure), corticosteroids, and/or anti-bacterial, antiviral, or anti-fungal agents.
- Alexander's ear deformity, hypertelorism, Jervell-Lange Nielso ⁇ , Refsum ' s and Usher's sydromes are found in approximately 20% of patients with sensorineural hearing loss.
- Congenital ear malformations may result from defects in the development of the membranous labyrinthine, the osseous labyrinthine, or both.
- profound hearing loss and vestibular function are found in approximately 20% of patients with sensorineural hearing loss.
- hereditary deformities may also be associated with other dysfunctions, including development of recurring menigitis, cerebral spinal fluid (CSF) leaks, as well as perilymphatic fistulas. Treatment of chronic infections are necessitated in hereditary disorder patients.
- CSF cerebral spinal fluid
- Otitis media which includes acute otitis media (AOM), otitis media with effusion (OME) and chronic otitis media as examples, is a condition affecting both adults and children.
- OM susceptibility is multifactorial and complex, including environmental, microbial and host factors. Bacterial infection accounts for a large percentage of OM cases, with more than 40% of cases attributed to Streptococcus pneumoniae infection. However, viral caxiscs, as well as other microbial agents, may also account for OM conditions.
- IL-I ⁇ , IL-6 and TNF- ⁇ are acute-phase cytokines that promote acute inflammatory response after infection with viruses and bacteria.
- Genetic studies supports this link between cytokines and OM by demonstrating a correlation in the occurrence of TNF- ⁇ SNP (single-nueleotide polymorphisms) and an increased susceptibility for OM in pediatric patients suffering from AOM and with a subsequent need for placement of tympanostomy tubes. (Patel et al. Pediatrics (2006) i 18:2273-2279).
- TNF- ⁇ and interleukins levels were found to increase in early developmental phase of OM, with TNF- ⁇ levels steadily increasing 12 hours after mnoculation.
- TNF- ⁇ levels steadily increasing 12 hours after mnoculation.
- liigher TNF- ⁇ levels have been associated with a history of multiple tympanostomy tube placements, indicating a role for TNF- ⁇ in chronic OM cases.
- direct injection of TNF- ⁇ and interle ⁇ kins has been shown to induce middle ear inflammation in a guinea pig model.
- OM can be caused by a virus, bacteria or both, it is often difficult to identify the exact cause and thus the most appropriate treatment.
- Treatment options of OM in the auris media include treatment with antibiotics, such as amoxicillin, clavulanate acid, trimethoprim- suliamethoxazole, cefuroxime. clarithromycin and azithromycin and other cephalosporins, macrolides, penicillins or sulfonamides.
- Surgical intervention is also available, including a myringotomy, an operation to insert a tympanostomy tube through the tympanic membrane and into the patient's middle ear to drain the fluid and balance the pressure between the outer and middle ear.
- Antipyretics and analgesics may also be prescribed to treat accompanying fever or pain effects.
- Pre-treatment with TNF- ⁇ inhibitors in experimental lipopolysaccharide (LPS)-induced OM animal models has been shown to suppress development of OM, suggesting a role in the treatment of OM or OME.
- treatment of such conditions include use of TNF-oc inhibitors in combination with other inflammatory response mediators, including platelet activating factor antagonists, nitric oxide synthase inhibitors and histamine antagonists.
- methotrexate, cyclophosphamide, and thalidomide are all cytotoxic small molecule agents that are systemically administered to treat ⁇ 1ED.
- the compounds are useful in the compositions and formulations disclosed herein for the treatment of inflammatory disorders of the auris media, including OM, by having a direct anti-inflammatory effect, particularly by interfering with TNF activity.
- metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of methotrexate, cyclophosphamide, and thalidomide that retain the ability of the parent cytotoxic agents to treat inflammatory disorders of the auris media, including OM, are useful in the formulations disclosed herein for the treatment of inflammatory disorders of the auris media, including OM.
- preferred metabolites of cyclophosphamide for incorporation into the compositions and formulations disclosed herein include 4- hydroxycyclophosphamide, aldophosphamide, phosphoramide mustard, or combinations thereof.
- Otitis externa also referred to as swimmer ' s ear
- OE is an inflammation and/or infection of the external ear.
- Oh is often caused by bacteria in the outer ear, which establish infection following damage to the skin of the ear canal.
- Primary bacterial pathogens that cause OE are Pseudomonas aeruginosa and Staphylococcus aureus, but the condition is associated with the presence of many other strains of gram positive and negative bacteria.
- OE is also sometimes caused by fungal infection in the outer ear, including Candida albicans and Aspergillus. Symptoms of OE include otalgia, swelling, and otorrhea. If the condition progresses significantly, OE may cause temporary conductive hearing loss as a result of the swelling and discharge.
- Treatment of OE involves eliminating the aggravating pathogen from the ear canal and reducing inflammation, which, is usually accomplished by administering combinations of antimicrobial agents, e.g., antibacterial and antifungal agents, with anti-inflammatory agents, e.g., steroids.
- antimicrobial agents e.g., antibacterial and antifungal agents
- anti-inflammatory agents e.g., steroids.
- Typical antibacterial agents for the treatment of OE include aminoglycosides (e.g., neomycin, gentamycin, and tobramycin), polymyxins (e.g., polymyxin B), fluoroquinolone (e.g., ofloxacin and ciprofloxacin), cephalosporins (e.g., eefuroxkne, ceflacor, cefprozil, loracarbef, cefmdir, eefixime, cefpodoxime proxetil, cefibutcn, and ceftriaxone), penicillins (e.g., amoxicillin, amoxicillin-clavulanate, and penicillinase-resistant penicillins), and combinations thereof.
- aminoglycosides e.g., neomycin, gentamycin, and tobramycin
- polymyxins e.g., polymyxin B
- fluoroquinolone
- Typical antifungal agents for the treatment of OE include clotrimazole, thimerasol, M-cresyl acetate, tolnaftate, itraconazole, and combinations thereof.
- Acetic acid is also administered to the ear, alone and in combination with other agents, to treat bacterial and fungal infections.
- Ear drops are often used as the vehicle for administration of the active agents. In the case that ear swelling has progressed substantially and ear drops do not penetrate significantly into the ear canal, a wick can be inserted into the ear canal to facilitate penetration of the treatment solutions.
- Oral antibiotics are also administered in the case of extensive soft tissue swelling that extends to the face and neck.
- topical ear drops such as ear drops containing neomycin
- ear drops containing neomycin are safe and effective for use in die ear canal, but can be irritating and even ototoxic to the auris media, prompting concern that such topical preparations should not be used unless the tympanic membrane is known to be intact.
- Utilization of the formulations disclosed herein for the treatment of OE allows for use of active agents that are potentially damaging to the auris media, even when the tympanic membrane is not intact.
- the controlled release formulations disclosed herein can be applied locally in the external ear with improved retention time, thus eliminating concern that the active agents will leak out of the ear canal into the amis media.
- otoprotectants can be added when ototoxic agents, such as neomycin, are used.
- compositions disclosed herein have increased retention time in the ear canal as a result of the formulation technology, thus eliminating the need for a device to maintain their presence in the outer ear.
- the formulations can be applied in the outer ear with a needle or ⁇ in ear dropper, and the active agents can be maintained at the site of inflammation without the aid of an ear wick.
- the treatment of OE with antimicrobial formulations disclosed herein encompasses the treatment of granular myringitis, a specific form of OE characterized by chronic infJamination of the pars tensa of the tympanic membrane.
- the outer epithelial and underlying fibrous layers of the tympanic membrane are replaced by a proliferating granulation tissue.
- the predominant symptom is foul-smelling otorrhea
- a variety of bacteria and fungi cause the condition, including Proletm and Psuedomonas species.
- antimicrobial agent formulations disclosed herein comprising antibacterial or antifungal agents are useful for the treatment of granular myringitis.
- the treatment of OE with antimicrobial formulations disclosed herein encompasses the treatment of chronic stenosing otitis externa.
- Chronic stenosing otitis externa is characterized by repeated infections, typically caused by bacteria or fungi. The primary symptoms are pruritus in the ear canal, otorrhea, and chronic swelling.
- Antimicrobial agent formulations disclosed herein comprising antibacterial or antifungal agents are useful for the treatment of chronic stenosing otitis externa.
- the treatment of OB with antimicrobial formulations disclosed herein encompasses the treatment of malignant or necrotizing external otitis, an infection involving the temporal and adjacent bones.
- Malignant external otitis is typically a complication of external otitis. It occurs primarily in persons with compromised immunity, especially in older persons with diabetes mellitus. Malignant external otitis is often causal by the bacteria Pseudomonas aeruginosa.
- antimicrobial agent formulations disclosed herein are useful for the treament of malignant or necrotizing external otitis.
- Otitis media which includes acute otitis media (AOM).
- OM susceptibility is multifactorial and complex, including environmental, microbial and host factors. Bacterial infection accounts for a large percentage of OM cases, with more than 40% of cases attributed to Streptococcus pneumoniae infection. However, viruses, as well as other microbes, may also account for OM conditions.
- OM can be caused by a virus, bacteria or both, it is often difficult to identify the exact cause and thus the most appropriate treatment.
- Treatment options for OM include antibiotics, such as penicillins (e.g., amoxicillin and amoxicillin-clavulanate), clavulanate acid, trimethoprim- sulfamethoxazole, cephalosporins (e.g., cefuroxirne, valacor, cefprozil, loracarbef, cefindir, cefixime, cefpodoxime proxetil, cefibuten, and ceftriaxone), maerolides and azalides (e.g., erythromycin, clarithromycin, and azithromycin), sulfonamides, and combinations thereof.
- antibiotics such as penicillins (e.g., amoxicillin and amoxicillin-clavulanate), clavulanate acid, trimethoprim- sulfameth
- Surgical intervention is also available, including myringotomy, an operation to insert a tympanostomy tube through the tympanic membrane and into the patient's middle ear to drain the fluid and balance the pressure between the outer and middle ear.
- Antipyretics and analgesics including benzocaine. ibuprofen and acetaminophen., may also be prescribed to treat accompanying fever or pain effects. J00192 ⁇ Regardless of the causative agent, increases in cytokine production, including interleukins and TNF, have been observed in the effluent media of individuals afflicted with OM.
- IL-I ⁇ , 1L-6 and TNF- ⁇ are acute-phase cytokines that promote acute inflammatory response after infection with viruses and bacteria.
- higher TNF- ⁇ levels have been associated with a history of multiple tympanostomy tube placements, indicating a role for TNF- ⁇ in chronic OM cases.
- direct injection of TNF- ⁇ and interleukins has been shown to induce middle ear inflammation in a guinea pig model.
- These studies support the role that cytokines may play in the origin and maintenance of OM in the auris media.
- treatment of OM includes the use of antimicrobial agents in conjunction with anti-inflammatory agents to eliminate the pathogen and treat the symptoms of inflammation.
- Such treatments include use of steroids, TNF- ⁇ inhibitors, platelet activating factor antagonists, nitric oxide synthase inhibitors, histamine antagonists, and combinations thereof in conjunction with the antimicrobial formulations disclosed herein.
- Mastoiditis is an infection of the mastoid process, which is the portion of the temporal bone behind the ear. It is typically caused by untreated acute otitis media. Mastoiditis are acute or chronic. Symptoms include pain, swelling, and tenderness in the mastoid region, as well as otalgia, erythematous, and otorrhea. Mastoiditis typically occurs as bacteria spread from the middle ear to the mastoid air cells, where the inflammation causes damage to the bony structures. The most common bacterial pathogens are Streptococcus pneumoniae, Streptococcus pyogenes,
- antimicrobial agent formulations disclosed herein comprising antibacterial agents effective against the bacteria are useful for the treatment of mastoiditis, including acute mastoiditis and chronic mastoiditis.
- Bullous myringitis is an infection of the tympanic membrane, caused by a variety of bacteria and viruses, including Mycoplasma bacteria. The infection leads to inflammation of the tympanic membrane and nearby canal, and causes the formation of blisters on the ear drum. The primary symptom of Bullous myringitis is pain, which, are relieved through the administration of analgesics.
- Antimicrobial formulations disclosed herein comprising antibacterial and antiviral agents are useful for the treatment of Bullous myringitis.
- Eustachian tubal catarrh or Eustachian salpingitis
- Eustachian tubal catarrh is caused from inflammation and swelling of the Eustachian tubes, resulting in a build-up of catarrh.
- antimicrobial formulations disclosed herein are useful for the treatment of Eustachian salpingitis.
- Labyrinthitis e.g., serous labyrinthitis
- the primary symptom is vertigo, bm the condition is also characterized by hearing loss, tinnitus, and nystagmus.
- Labrynthitis maybe acute, lasting for one to six weeks and being accompanied by severe vertigo and vomiting, or chronic, with symptoms lasting for months or even years.
- Labyrinthitis is typically caused by viral or bacterial infection.
- antimicrobial formulations disclosed herein comprising antibacterial and aniiviral agents are useful for the treatment of labyrinthitis.
- Facial nerve neuritis is a form of neuritis, an inflammation of the peripheral nervous system, afflicting the facial nerve.
- the primary symptoms of the condition are a tingling and burning sensation, and stabbing pains in the affected nerves. In severe cases, there are numbness, loss of sensation, and paralysis of the nearby muscles.
- the condition is typically caused by herpes zoster or herpes simplex viral infection, but has also been associated with bacterial infection, e.g., leprosy.
- antimicrobial formulations disclosed herein comprising antibacterial and antiviral agents are useful for the treatment of facial nerve neuritis.
- antimicrobial formulations disclosed herein are also useful for the treatment of temporal bone osteoradionecrosis.
- Kinetosis also known as motion sickness, is a condition in which there is a disconnection between visually perceived movement and the vestibular system's sense of movement. Dizziness, fatigue, and nausea are the most common symptoms of kinetosis. Dimenhydrinate, cinnarizine, and meclizine are all systemic treatments for kinetosis. Additionally, benzodiazepines and antihistamines have demonstrated efficacy in treating kinetosis.
- Labyrinthitis is an inflammation of the labyrinths of the ear which contain the vestibular system of the inner ear. Causes include bacterial, viral, and fungal infections. Tt may also be caused by a head injury or allergies. Symptoms of labyrinthitis include difficulty maintaining balance, dizziness, vertigo, tinnitus, and hearing loss. Recovery may take one to six weeks; however, chronic symptoms are present for years.
- Prochlorperazine is often prescribed as an antiemetic. Serotonin-reuptake inhibitors have been shown to stimulate new neural growth within the inner ear. Additionally, treatment with antibiotics is prescribed if the cause is a bacterial infection, and treatment with corticosteroids and anlivirals is recommended if the condition is caused by a viral infection.
- MaI de debarquement is a condition which usually occurs subsequent to a sustained motion event, for example, a cruise, car trip, or airplane ride. It is characterized by a persistent sense of motion, difficulty maintaining balance, fatigue, and cognitive impairment. Symptoms may also include dizziness, headaches, hyperaeusis, and'or tinnitus. Symptoms often last in excess of a month. Treatment includes benzodiazepines, diuretics, sodium channel blockers, and tricyclic antidepressants.
- Microvascular compression syndrome also called “vascular compression” or “neurovascular compression”
- MCS Microvascular compression syndrome
- vascular compression also called “vascular compression” or “neurovascular compression”
- vascular compression is a disorder characterized by vertigo and tinnitus. It is caased by the irritation of Cranial Nerve VIl by a blood vessel.
- Other symptoms found in subjects with MCS include, but are not limited to, severe motion intolerance, and neuralgic like "quick spins”.
- MOS is treated with carbamazepine. TRILEPT AIJS ) , and baclofen. It can also be surgically treated.
- microbial infections are known to cause cochleovestibular disorders, including hearing loss.
- infections include rubella, cytomegalovirus, mononucleosis, varicella zoster (chicken pox), pneumonia, Borrelia species of bacteria (Lyme disease), and certain fungal infections.
- controlled release antimicrobial agent formulations disclosed herein are also used for localized treatment of these infections in the ear.
- Free radicals are highly reactive atoms, molecules, or ions the reactivity of which results from the presence of unpaired electrons.
- Reactive oxygen species form as a result of sequential reduction of molecular oxygen .
- reactive oxygen species of interest include, but are not limited to, superoxide, hydrogen peroxide, and hydroxyl radicals.
- ROS are naturally produced as a by-product of the production of ATP. ROS can also result from the use of cisplatin, and aminoglycosides. Further, stress to stereocila caused by acoustic trauma results in otic hair cells producing ROS.
- ROS can damage cells directly by damaging nuclear DNA and mitochondrial DNA, Damage to the former can lead to mutations which impair the functioning of auditory cells and/or apoptosis. Damage to the latter often results in decreased energy production and increased ROS production both of which can lead to impaired cellular functioning or apoptosis. Further, ROS can also damage or kill ceils by oxidizing the polydesaturated fatty acids which comprise lipids, oxidizing the amino acids which comprise proteins, and oxidizing co-factors necessary for the activity of enzymes. Antioxidants can ameliorate damage by caused by ROS by preventing their formation, or scavenging the ROS before they can damage the cell.
- Damage to ⁇ nitochondria by ROS is often seen in hearing loss, especially healing loss due to aging.
- the loss of ATP correlates to a loss in neural functioning in the inner ear. It can also lead to physiological changes in the inner ear.
- damage to mitochondria often results in an increased rate of cellular degradation and apoptosis of inner ear cells.
- the cells of the stria vascularis are the most metabolically active due to the vast, energy requirements needed to maintain the ionic balance of fluids in the inner ear. Thus, the cells of the stria vascularis are most often damaged or killed due to damage of the mitochondria.
- Otosclerosis is an abnormal growth of bone in the middle ear, which prevents structures within the ear from transducing vibration, which causes hearing loss.
- Otoscelorosis usually effects the ossicles, in particular the stapes, which rests in the entrance to the cochlea in the ova! window.
- the abnormal bone growth fixates the stapes onio the oval window, preventing sound passing waves from traveling to the cochlea.
- Otoscelorosis may cause a sensorineural hearing loss, i.e. damaged nerve fibers or hearing hair cells, or conductive hearing loss.
- Treatment of otoscelrosis may include surgery to remove the fixated stapes bone, called a stapedectomy. Fluoride treatment may also be used, which will not reverse the hearing loss but may slow the development of otoscelorosis.
- Ototoxicity refers to hearing loss caused by a toxin.
- the hearing loss are due to trauma to otic hair cells, the cochlea, and/or the cranial nerve VD.
- Multiple drugs are known to be ototoxic. Often ototoxicity is dose-dependent. It are permanent or reversible upon withdrawal of the drug.
- 002ll]Known ototoxic drugs include, but are not limited to, the aminoglycoside class of antibiotics (e.g. gentamicin, and amikacin), some members of the rnacrolide class of antibiotics (e.g erythromycin), some members of the glycopeptide class of antibiotics (e.g.
- vancomycin vancomycin
- salicylic acid nicotine
- chemotherapeutic agents e.g. actinomycin, bleomycin, cisplatin, carbopiatin and vincristine
- members of the loop diuretic family of drugs e.g. furoseraide
- Cispiatin and the aminoglycoside class of antibiotics induce the production of reactive oxygen species ("ROS").
- ROS can damage cells directly by damaging DNA, polypeptides, and/or lipids.
- Antioxidants prevent damage of ROS by preventing their formation or scavenging free radicals before they can damage the cell.
- Both cisplatin and the aminoglycoside class of antibiotics are also thought to damage the ear by binding melanin in the stria vascularis of the inner ear.
- Salicylic acid is classified as ototoxic as it inhibits the function of the polypeptide prestin. Prestin mediates outer otic hair cell motility by controlling the exchange of chloride and carbonate across the plasma membrane of outer otic hair cells. It is only found in the outer otic hair cells, not the inner otic hair cells. Accordingly, disclosed herein is the use of controlled release auris- compositions comprising antioxidants to prevent, ameliorate or lessen ototoxic effects of chemotherapy, including but not limited to cisplatin treatment, aminoglycoside or salicylic acid administration, or other ototoxic agents.
- Postural vertigo otherwise known as positional vertigo, is characterized by sudden violent vertigo that is triggered by certain head positions. This condition are caused by damaged semicircular canals caused by physical injury Io the auris interna, otitis media, ear surgery or blockage of the artery to the auris interna.
- Vertigo onset in patients with postural vertigo usually develops when a person lies on one ear or tilts the head back to look up. Vertigo is accompanied by nystagmus. In severe cases of postural vertigo, the vestibular nerve is severed to the affected semicircular canal. Treatment of vertigo is often identical to Meniere's disease, and may include meclizine, lorazepam,
- Fluids and electrolytes may also be intravenously administered if the vomiting is severe.
- Presbycusis (or presbyacusis or age related hearing loss (.MtHL)) is the progressive bilateral loss of hearing that results from aging. Most hearing loss occurs at higher frequencies (i.e.
- Hie disorder is most often treated by the implantation of a hearing aid and/or the administration of pharmaceutical agents which prevent the build up of ROS. ⁇ 0 ⁇ 217J The disorder is caused by elianges in the physiology of the inner ear, the middle ear, and/or die VlI nerve.
- Changes in the inner ear resulting in presbycusis include epithelial atrophy with loss of otic hair cells and/or stereocilia, atrophy of nerve cells, atrophy of (he stria vascularis, and the thickening/stiffening of the basilar membrane. Additional changes wliich can contribute to presbycusis include the accumulation of defects in the tympanic membrane and the ossicles.
- Presbycusis occurs as a part of normal aging, and occurs as a result of degeneration of the receptor cells in the spiral Organ of Corti in the auris interna. Other causes may also be attributed to a decrease in a number of nerve fibers in the vestibulocochlear nerve, as well as a loss of flexibility of the basilar membrane in the cochlea.
- Treatment regimens have been proposed, including treatment with antioxidants such as alpha lipoic acid.
- [00220 ⁇ Ramsay Hunt's syndrome is caused by a herpes zoster infection of the auditory nerve.
- the infection may cause severe ear pain, hearing loss, vertigo, as well as blisters on the outer ear, in the ear canal, as well as on the skin of the face or neck supplied by the nerves. Facial muscles may also become paralyzed if the facial nerves are. compressed by the swelling. Hearing loss are temporary or permanent, with vertigo symptoms usually lasting from several days to weeks.
- Treatment of Ramsay Hunt's syndrome includes administration of antiviral agents, including acyclovir.
- Other antiviral agents include famciclovir and valacyclovir.
- Combination of antiviral and corticosteroid therapy may also be employed to ameliorate herpes zoster infection.
- Analgesics or narcotics may also be administered to relieve the pain, and diazempam or other central nervous system agents to suppress vertigo. Capsaicin, lidocaine patches and nerve blocks may also be used. Surgery may also be performed on compressed facial nerves to relieve facial paralysis.
- [0 ⁇ 222J Recurrent vestibulopathy is a condition wherein the subject experiences multiple episodes of severe vertigo. The episodes of vertigo may last for minutes or hours. Unlike Meniere's Disease, it is not accompanied by hearing loss. In some cases it may develop into Meniere's Disease or Benign Paroxysmal Positional Vertigo. Treatment is similar to that of Meniere's Disease.
- Syphilis is a venerea] disease, caused by the spirochete Treponema pallidum, which in its secondary and tertiary stages may result in auditory and vestibular disorders due to membranous labyrinthis. and secondarily include meningitis.
- cochieovestibular disorders resulting from syphilis are often similar to those of other otic disorders, such as AIED and Meniere's disease, and include tinnitus, deafness, vertigo, malaise, sore throat, headaches, and skin rashes.
- Syphilis infection may lead to congenital prenatal hearing loss, affecting approximately 11.2 per 100,000 live births in the United States, as well as sudden bearing loss in adults.
- Treatment of otosyphilis typically includes a combination of steroids (e.g., prednisolone) and antibacterial agents (e.g., benzathine penicillin G (BICILLIN LA®), penicillin G procaine, doxycyeline, tetracycline, ceftriaxone, azithromycin).
- steroids e.g., prednisolone
- antibacterial agents e.g., benzathine penicillin G (BICILLIN LA®), penicillin G procaine, doxycyeline, tetracycline, ceftriaxone, azithromycin.
- the temporal bone which contains part of the ear canal, the middle ear and the auris interna, is subject to fractures from blows to the skull or other injuries. Bleeding from the ear or patchy bruising is symptomatic of a fracture to the temporal bone, and may a computed tomography (CT) scan for accurate diagnosis. Temporal bone fractures may rupture the eardrum, causing racial paralysis and sensorineural hearing loss.
- CT computed tomography
- Treatment of detected temporal bone fractures includes an antibiotic regimen to prevent meningitis, or an infection of brain tissue. Tn addition, surgery are performed to relieve any subsequent pressure on the facial nerve due to swelling or infection.
- TMD temporomandibular joint disease
- auris interna disorders Some evidence exists for a relationship between temporomandibular joint disease (TMD) and auris interna disorders.
- Anatomical studies demonstrate the possible involvement of the trigeminal nerve, where trigemminal innervation of the vascular system has been shown to control cochlear and vestibular labyrinth function. (V ass et al. Neuroscience (19.98) 84:559-567).
- projections of ophthalmic fibers of the trigeminal Gasser ganglion to the cochlea through the basilar and anterior inferior cerebellar arteries can play an important role in the vascular tone in quick vsaodilatatory response to metabolic stresses, e.g. intense noise.
- Auris interna diseases and symptoms such as sudden hearing loss, vertigo and tinnitus, may originate from reduction of the cochlear blood flow due to the presence of abnormal activity in the trigeminal ganglion, for example from migrane or by the central excitatory effect originated in chronic or deep pain produced by TMD.
- forceful muscle contractions in TMD may elicit modulations in the neurological and auditory and equilibrium function.
- the auditory and vestibular modulations may occur as a result of hyerptonicity and muscular spasm, which in turn irritates nerves and blood vessels that affect auris interna function by nwscular trapping.
- Relief of the affected nerve or muscular contractions may act to relieve auditory or vestibular symptoms.
- Medications including barbiturates or diazepam, may thus relieve auditory or vestibular dysfunction in TMD patients.
- the utricle is one of the two otoliths found in the vestibular labyrinth. It is responsive to both gravity and linear acceleration along the horizontal plane. Utricular dysfunction is a disorder caused by damage to the utricle. It is often characterized by a subject's perception of tilting or imbalance.
- vertigo is described as a feeling of spinning or swaying while the body is stationary. There are two types of vertigo. Subjective vertigo is the false sensation of movement of the body.
- Objective vertigo is the perception that one's surrounding are m motion. It is often accompanied by nausea, vomiting, and difficulty maintaining balance.
- vertigo is caused by an over-accumulation of fluid in the endolymph. This fluid imbalance results in increased pressure on the cells of the inner ear which leads to the sensation of movement.
- the most common cause of vertigo is benign paroxysmal positional vertigo, or BPPV. It can also be brought on by a head injury, or a sudden change of blood pressure. It is a diagnostic symptom of several diseases including superior canal dehiscence syndrome.
- Vestibular neuronitis or vestibular neuropathy, is an acute, sustained dysfunction of the peripheral vestibular system. It is theorized that vestibular neuronitis is caused by a disruption of afferent neuronal input from one or both of the vestibular apparatuses. Sources of this disruption include viral infection, and acute localized ischemia of the vestibular nerve and/or labyrinth.
- Vestibular neuronitis is characterized by sudden vertigo attacks, wl ⁇ ch may present as a single attack of vertigo, a series of attacks, or a persistent condition which diminishes over a matter of weeks. Symptoms typically include nausea, vomiting, and presdous upper respiratory tract infections, although there are generally no auditory symptoms.
- the first attack of vertigo is usually severe, leading to nystagmus, a condition characterized by flickering of the eyes involuntarily toward the affected side. Hearing loss does not usually occur.
- vestibular neuronitis is caused by inflammation of the vestibular nerve, the nerve that connects the inner ear to the brain, and is likely caused by viral infection. Diagnosis of vestibular neuronitis usually involves tests for nystagmus using electronystamography, a method of electronically recording eye movements. Magnetic resonance imaging may also be performed to determine if other causes may play a role in the vertigo symptoms.
- Treatment of vestibular neuronitis typically involves alleviating the symptoms of the condition, primarily vertigo, until the condition clears on its own. Treatment of vertigo is often identical to Meniere's disease, and may include meclizine, lorazepam, prochlorperazine, or scopolamine. Fluids and electrolytes may also be intravenously administered if the vomiting is severe. Corticosteroids, such as prednisilone, are also given if the condition is detected early enough.
- compositions disclosed herein comprising an antiviral agent can be administered for the treatment of vestibular neuronitis. Further, the compositions are administered with other agents that are typically used to treat symptoms of the condition, including anticholinergics, antihistamines, benzodiazepines, or steroids. Treatment of vertigo is identical to Meniere's disease, and may include meclizine, lorazepam, prochlorperazine or scopolamine. Fluids and electrolytes may also be intravenously administered if the vomiting is severe.
- Hl -receptor antagonists such as dimenhydrinate, diphenhydramine, meclizine, and prometliazine, dimmish vestibular stimulation and depress labyrinthine function through anticholinergic effects.
- Benzodiazepines such as diazepam and lorazepam, are also used to inhibit vestibular responses due to their effects on the
- Anticholinergics for example scopolamine, are also prescribed. They function by suppressing conduction in the vestibular cerebellar pathways.
- corticosteroids i.e.
- prednisone are prescribed to ameliorate the inflammation of the vestibular nerve and associated apparatus.
- auris media and/or auris interna structures Access to, for example, the vestibular and cochlear apparatus will occur through the auris media including the round window membrane, the oval window/stapes footplate, the annular ligament and through the. otic capsule/temporal bone.
- auris media and/or auris interna also affords the use of previously imdesired therapeutic agents, including agents with poor PK profiles, poor uptake, low systemic release and/or toxicity issues.
- otic agent formulations and compositions As well as the biological faiood barrier present in the auris interna, the risk of adverse effects will be reduced as a result of treatment with previously characterized toxic or ineffective otic active agents, (e.g., irnmunomodulatory agents such as anti-TNF agents).
- toxic or ineffective otic active agents e.g., irnmunomodulatory agents such as anti-TNF agents.
- a controlled release otic agent formulation e.g., immurtomodulating agent or auris pressure modulator formulation
- a constant, variable and/or extended source of an otic agent is provided to the individual or patient suffering from an otic disorder, reducing or eliminating the variability of treatment.
- one embodiment disclosed herein is to provide a formulation that enables at least one therapeutic agent to be released in therapeutically effective doses either at variable or constant rates such as to ensure a continuous release of the at least one agent.
- the auris active agents disclosed herein are administered as an immediate release formulation or composition.
- the auris active agents are administered as a controlled release formulation, released either continuously or in a pulsatile manner, or valiants of both.
- the active agent formulation is administered as both an immediate release and controlled release formulation, released either continuously or in a pulsatile manner, or variants of both. The release is optionally dependent on environmental or physiological conditions, for example, the external ionic environment (see, e.g. Oros* release system, Johnson & Johnson).
- auris media and/or auris interna agents in combination with the otic agent formulations and compositions disclosed herein.
- such agents assist in the treatment of hearing or equilibrium loss or dysfunction as a result of an autoimmune disorder, including vertigo, tinnitus, hearing loss, balance disorders, infections, inflammatory response or combinations thereof.
- agents that ameliorate or reduce the effects of vertigo, tinnitus, hearing loss, balance disorders, infections, inflammatory response or combinations thereof are also contemplated to be used in combination with the otic agents described herein including steroids, anti-emetic agents, local anesthetic agents, corticosteroids, cheinotherapeutic agents, including Cytoxan, azathiaprine or methotrexate; treatment with collagen, gamma globulin, interferons, Copaxone, central nervous system ageots, antibiotics, platelet-activating factor antagonists, nitric oxide synthase inhibitors and combinations thereof.
- the auris-compatible pharmaceutical compositions or formulations included herein also include carriers, adjuvants, such as preserving, stabilizing, wetting or emulsifying agents, solution promoters, salts for regulating the osmotic pressure, and/or buffers.
- carriers, adjuvants, and other excipients will be compatible with the environment in the auris media and/or auris interna. Accordingly, specifically contemplated are carriers, adjuvants and excipients that lack ototoxicity or are minimally ototoxic in order to allow effective treatment of the otic disorders contemplated herein with minimal side effects in the targeted regions or areas.
- otic pharmaceutical compositions or formulations disclosed herein are optionally targeted to distinct regions of the auris media and/or auris interna, including but not limited to the tympanic cavity, vestibular bony and membranous labyrinths, cochlear bony and membranous labyrinths and other anatomical or physiological structures located within the auris interna.
- otic compositions suitable for the treatment of any otic condition, disease or disorder (e.g., middle and/or inner ear disorder) described herein, comprising
- an auris formulation described herein administered to an individual or patient in need thereof.
- the formulations described herein are suitable for the treatment of any disease described herein.
- the treatment is long-term treatment for chrome recurring disease.
- the treatment is prophylactic administration of an otic formulation described herein for the treatment of any otic disease or disorder described herein.
- prophylactic administration avoids ocurrence of disease in individuals suspected of having a disease or in individuals genetically predisposed to an otic disease or disorder.
- the treatment is preventive maintenance therapy.
- preventive maintenance therapy avoids recurrence of a disease.
- compositions described herein are safe for long-term adrainstration.
- the auris compositions described herein have very low ototoxicity and provide a steady sustained release of a therapeutic agent for a period of at least one week, two weeks, three weeks or a month.
- compositions and formulations to treat and'or prevent diseases associated with the ear including the cochlea, the middle ear and inner ear, including autoimmune inner ear disorder (AlED), Meniere's disease (endolymphatic hydrops), noise induced hearing loss (NIHL), sensorineural hearing loss (SNL), tinnnitus, otosclerosis, balance disorders, vertigo and the like.
- AlED autoimmune inner ear disorder
- Meniere's disease endolymphatic hydrops
- NIHL noise induced hearing loss
- SNL sensorineural hearing loss
- tinnnitus otosclerosis
- balance disorders vertigo and the like.
- the etiology of several ear diseases or disorders consists of a syndrome of progressive hearing loss, including noise induced hearing loss and age-related hearing loss, dizziness, nausea, nystagmus, vertigo, tinnitus, inflammation, swelling, infection and/or congestion. These disorders may have many causes, such as infection, exposure to noise, injury, inflammation, tumors and/or adverse response to drugs or other chemical agents.
- Several causes of hearing and/or equilibrium impairment are attributed to inflammation and/or an autoimmune disorder and/or a cytokine- mediated inflammatory response,
- control release imrnunomodulator compositions and formulations to treat inflammation or infection of the auris media, including otitis media.
- a few therapeutic products are available for the treatment of AIED, including anti-TNF agents; however, systemic routes via oral, intravenous or intramuscular routes are currently used to deliver these therapeutic agents.
- aural pressure modulating compositions and formulations to treat fluid homeostasis disorders of the inner ear, including Meniere's Disease, endolymphatic hydrops, progressive hearing loss, including noise induced hearing loss and age- related hearing loss, dizziness, vertigo, tinnitus and similar conditions.
- the compositions provided herein are CNS modulating compositions and formulations to treat tinnitus, progressive hearing loss, including noise induced hearing loss and age-related hearing loss, and balance disorders.
- Balance disorders include benign paroxysmal positions vertigo, dizziness, endolymphatic hydrops, kinetosis, labyrinthitis, MaI de debarquement, Meniere's Disease, Meniere's Syndrome, myringitis, otitis media, Ramsay Hunt's Syndrome, recurrent vestibulopathy, tinnitus, vertigo, microvascular compression syndrome, utricular dysfunction, and vestibular neuronitis.
- GABA A receptor modulators and local anesthetics.
- the compositions provided herein are cytotoxic agent compositions and formulations for the treatment of autoimmune diseases of the ear. including autoimmune inner ear disease (AlED). Also provided herein are controlled release cytotoxic agent compositions for the treatment of disorders of the auris media, including otitis media.
- the compositions disclosed herein are also useful for the treatment of cancer, particularly cancer of the ear A few therapeutic products are available for the treatment of AlED, including certain cytotoxic agents.
- the cytotoxic agents methotrexate and cyclophosphamide have been tested and are used for systemic treatment of AIED.
- thalidomide while not currently administered for the treatment of AIED. has been used to treat Behcet's disease, which is often associated with AIED.
- compositions provided herein comprise auris sensory cell modulators for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- auris sensory cell modulating agent compositions and formulations to treat ototoxicity, excitotoxicity, sensorineural hearing loss, Meniere's Disease/Syndrome, endolymphatic hydrops, labyrinthitis, Ramsay Hunt's Syndrome, vestibular neuronitis and microvascular compression syndrome.
- compositions provided herein are antimicrobial agent compositions mid formulations for the treatment of otic disorders, including otitis externa, otitis media, Ramsay Hunt syndrome, otosyphilis, AIED, Meniere's disease, and vestibular neuronitis.
- the compositions provided herein prevent, relieve, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals and/or the dysfunction of the mitochondria.
- compositions and formulations to treat fluid homeostasis disorders of the inner ca ⁇ including Meniere's Disease, endolymphatic hydrops, progressive hearing loss, including noise induced hearing loss and age- related hearing loss, dizziness, vertigo, tinnitus and similar conditions.
- Systemic routes via oral, intravenous or intramuscular routes are currently used to deliver ion channel modulating therapeutic agents.
- the otic compositions described herein w ⁇ l have pH and osraolarity that is auris-acceptable. Any otic composition described herein meets the stringent sterility requirements described herein and will be compatible with the endolymph and/or the perilymph.
- Pharmaceutical agents that are used in conjunction with the formulations disclosed herein include agents that ameliorate or lessen otic disorders, including auris interna disorders, and their attendant symptoms, which include but are not limited to hearing loss, nystagmus, vertigo, tinnitus, inflammation, swelling, infection and congestion.
- Otic disorders may have many causes, such as infection, injury, inflammation, tumors and adverse response to drugs or other chemical agents that are responsive to the pharmaceutical agents disclosed herein.
- a skilled practitioner would be familiar with agents that are useful in the amelioration or eradication of otic disorder; accordingly, agents which are not disclosed herein but are useful for the amelioration or eradication of otic disorders arc expressly included and intended within the scope of the embodiments presented.
- pharmaceutically active metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of the otic agents disclosed herein hatch retain the ability of the parent antimicrobial agents to treat otic disorders are useful in the formulations.
- Active ingredients or otic therapeutic agents include, but are not limited to, antiinflammatory agents, anti- antioxidants, neuroprotective agents, glulamate modulators, TNF ⁇ alpha modulators, interleukin 1 beta modulators, retinaldehyde modulators, notch modulators, gamma - secretase modulators, thalidomide, ion and/or flulid (e.g., water) homeostasis modulators, vasopressin inhibitors, inhibitors of the vasopressin-mediated AQP2 (aquaporin 2) system, transcriptional regulators of the inner-ear transcriptional regulatory network (including, e.g., transcriptional regulators of estrogen-related receptor beta), inner ear hair cell growth factors, including BDNF (brain derived and NF-3, and other therapeutic modalities.
- antiinflammatory agents include, but are not limited to, antiinflammatory agents, anti- antioxidants, neuroprotective agents, glulamate modulators, TNF ⁇ alpha modulators, interleukin 1 beta modulators
- Agents explicitly include an agonist of an otic target, a partial agonist of an otic target, an antagonist of an otic target, a partial antagonist of an otic target, an inverse agonist of an otic target, a competitive antagonist of an otic target, a neutral antagonist of an otic target, an orthosteric antagonist of an otic target, an allosteric antagonist of ao otic target a positive allosteric modulator of an otic target, or
- agents that produce systemic toxicities e.g., liver toxicity
- PK characteristics e.g. short half-life
- pharmaceutical agents which have been previously shown to be toxic, harmful or non-effective during systemic application, for example through toxic metabolites formed after hepatic processing, toxicity of the drug in pellicular organs, tissues or systems, through high levels needed to achieve efficacy, through the inability to be released through systemic pathways or through poor PK characteristics, are useful in some embodiments herein.
- the formulations disclosed herein are contemplated to be targeted directly to otic structures where treatment is needed; for example, one embodiment contemplated is the direct application of the aural pressure modulating formulations disclosed herein onto the round window membrane or the crista fenestrae cochlea of the auris interna, allowing direct access and treatment of the auris interna, or inner ear components.
- the aurai pressure modulating formulation disclosed herein is applied directly to the oval window.
- direct access is obtained through microinjection directly into the auris interna, for example, through cochlear nucroperrusion.
- Such embodiments also optionally comprise a drug delivery device, wherein the drug delivery device delivers the aural pressure modulating formulations through use of a needle and syringe, a pump, a microinjection device, an in situ forming spongy material or any combination thereof.
- any o ⁇ c agent formulation described herein is targeted to the auris media through piercing of the intratyrnpanic membrane and applying the otic agent formulation directly to the auris media structures affected, including the walls of the tympanic cavity or auditory ossicles.
- the auris active agent formulations disclosed herein are confined to the targeted auris media structure, and will not be lost, for example, through diffusion or leakage through the eustachian tube or pierced tympanic membrane.
- the auris-compatible formulations disclosed herein are delivered to the auris externa in any suitable manner, including by cotton swab, injection or ear drops.
- the otic formulations described herein are targeted to specific regions of the auris externa by application with a needle and syringe, a pump, a microinjection device, an in situ forming spongy material or any combination thereof.
- antimicrobial agent formulations disclosed herein are delivered directly to the ear canal, where they are retained, thereby reducing loss of the active agents from the target ear structure by drainage or leakage.
- agents which may have been previously rejected as, for example, an antimicrobial agent may find use herein because of the targeted nature of the embodiments which bypass systemic effects, including toxicity and harmful side effects.
- onercept a previously rejected anri-TNF agent due to toxicity and safety issues, is useful as an anti- TNF agent in some of the embodiments disclosed herein.
- Also contemplated within the scope of embodiments described herein is the administration of higher doses of pharmaceutical agents, for example agents that have dose limiting toxicities, compared to currently approved doses for such pharmaceutical agents
- Some pharmaceutical agents are ototoxic.
- some chemotherapeutic agents including actinomycin, bleomycin, cisplatin, carboplatin and vincristine; and antibiotics, including erythromycin, gentamicin, streptomycin, dihydrostreplomycin, tobramycin, netilmicin, amikacin, neomycin, kanamycin, etiomycin, vancomycin, metronidizole, capreomycin, are mildly to very toxic, and may affect the vestibular and cochlear structures differentially.
- the combination of an ototoxic drug, for example cisplatin, in combination with an antioxidant is protective and lessen the ototoxic effects of the drug.
- the localized application of the potentially ototoxic drug lessens the toxic effects that might otherwise occur through systemic application through the use of lower amounts with maintained efficacy, or the use of targeted amounts for a shorter period of time. Accordingly, a skilled practitioner choosing a course of therapy for targeted otic disorder will have the knowledge to avoid or combine an ototoxic compound, or to vary the amount or course of treatment to avoid or lessen ototoxic effects.
- excipients, diluents or carriers are potentially ototoxic.
- benzalkonium chloride a common preservative, is ototoxic and therefore potentially harmful if introduced into the vestibular or cochlear structures.
- the ototoxicity of the pharmaceutical agents. excipients, diluents, carriers, or formulations and compositions disclosed herein can be ascertained using an accepted animal model.
- a controlled release otic formulation includes otoprotective agents, such as antioxidants, alpha lipoic acid, calicum, fbsfomycin or iron chelators, to counteract potential ototoxic effects that may arise from the use of specific therapeutic agents or excipients, diluents or carriers.
- otoprotective agents such as antioxidants, alpha lipoic acid, calicum, fbsfomycin or iron chelators
- agents that are used in the embodiments disclosed herein, either alone or in combination with other auris interna agents include anti-apoptotic agents, including caspases, JNK. inhibitors (by way of example only CEP/KT-7515, AS601245, SPC9766 and SP600125), antioxidants, NSAlDs, neuroprotectants, glutamate modulators, interleukin 1 modulators, interleukin-1 antagonists, including tumor necrosis factor- ⁇ coverting enzyme (TACE) and caspases, retinaldehyde modulator, notch modulator, gamma secretase modulator, thalidomide, lalanoprost (Xalatan*) for reducing internal pressure and combinations thereof.
- anti-apoptotic agents including caspases, JNK. inhibitors (by way of example only CEP/KT-7515, AS601245, SPC9766 and SP600125), antioxidants, NSAlDs, neuroprotectants, glutamate modulators, interleukin
- agents which reduce or ameliorate symptoms or effects as a result of an autoimmune disease and/or inflammatory disorder including AIED or OM. Accordingly, some embodiments incorporate the use of agents which block the effects of TNF- ⁇ , including anti-TNF agents.
- anti-TNF agents include protein-based therapeutics, such as etanercept (ENBREL*), infliximab (REMICADE * * 1 ), adalimumab (HUMIRA*) and golimumab (CNTO 148), and small molecule therapeutics, such as TACE inhibitors, IKLK inhibitors or calcineurin inhibitors or combinations thereof,
- Infliximab and adalir ⁇ umab are anti-TNF monoclonal antibodies, and etanercept is a fusion protein designed to bind specifically to the TNF protein, AU are currently approved for use i « the treatment of rheumatoid arthritis.
- Golimumab which is currently in Phase 3 clinical trials for rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis, is a fully-humanized anti-TNF- alpha IgGl monoclonal antibody that targets and neutralizes both the soluble and the membrane- bound form of TNF- ⁇ .
- TNF receptors pegylated soluble TNF receptor type i; Amgen
- TNF binding factors Onercept; Serono
- TNF antibodies US Patent App. No. 2005/0123541 ; US Patent App. No. 2004/0185047
- single domain antibodies against the p55 TNF receptor US Patent App. No. 2008/00088713
- soluble TNF receptors US Patent App. No. 2007/0249538
- fusion polypeptides binding to TNF US Patent App. No. 2007/0128177
- flavone derivatives US Patent App. No. 2006/0105967
- onercept a soluble TNF p55 receptor
- Three phase-Ill clinical trials reported patients diagnosed with fatal sepsis. A risk, to benefit analysis was subsequently performed, resulting in the discontinuation of the clinical trials.
- the embodiments herein specifically contemplate the use of anti-TNF agents which have been previously shown to have limited or no systemic release, systemic toxicity, poor PK characteristics of combinations thereof.
- etanercept, infliximab and adalimumab are currently approved systemic therapies for use in rheumatoid arthritis, these anti-TNF agents are not without serious adverse side effects. It is contemplated that the localized application of the anti-TNF agents to the target, otic structures for treatment of autoimmune and/or inflammatory disorders will result in the reduction or elimination of these adverse side effects experienced with systemic treatment. Moreover, localized treatinent with the anti-TNF agents contemplated herein will also reduce the amount of agent needed for effective treatment of the targeted disorder due, for example, to the existence of the biological blood barrier in the a ⁇ ris interna or to the lack of sufficient systemic access to the auris media.
- Etanercept is a dimeric fusion protein consisting of the extracellular ligand-bindmg portion of the human 75 kilodalton (r>75) tumor necrosis factor receptor (TNFR) linked to the Fc portion of human IgGl.
- the Fc component of etanercept conta ⁇ is the C H 2 domain, the C H 3 domain and hinge region, but not the CHI domain of IgGl .
- Etanercept is a recombinant protein consisting of 934 amino acids, with an apparent molecular weight of approximlately 150 kilodaltons.
- Etanercept binds specifically to tumor necrosis factor (TNF), and acts by inhibiting the interaction of TNF with cell surface TNF receptors. Serious side effects with etanercepf have been reported with systemic administration, including serious infections and sepsis that resulted in fatalities.
- TNF tumor necrosis factor
- etanercept Other side effects observed upon intravenous administration of etanercept include contraction of tuberculosis; onset or exacerbation of central nervous system disorders, including mentai status changes, transverse myelitis, optic neuritis, multiple sclerosis and seizures resulting in permanent disability; adverse hematologic events, including pancytopenia, aplastic anemia with fatal outcomes, blood dyscrasias, persistent fever, bruising, bleeding and pallor, neutropenia and cellulitis. Treatment with etanercept may also result in the formation of autoantibodies, which may develop into a lupus-like syndrome, as well as development of malignant disorders.
- Infrequent side effects include heart failure, myocardial infarction, myocardial ischemia, hypertension, hypotension, deep vein thrombosis, thrombophlebitis, cholecystitis, pancreatitis, gastrointestinal hemorrhage, bursitis, polymyositis, cerebral ischemia, depression, dyspnea, pulmonary embolism, and membranous glomeralonephropathy in rheumatoid arthritis patients.
- Varicella infections, gastroenteritis, depression/personality disorder, cutnaeous ulcer, esophagitis/gastritis, group A streptococcal septic shock, type I diabetes meliitus, and soft tissue and post-operative wound infection was also seen in juvenille rheumatoid arthiritis patients.
- Infliximab is a chimeric human-mouse IgGlK monoclonal antibody with an approximate molecular weight of 149 kilodaltons. Infliximab binds specifically to TNFcc with an association constant of 10 i0 M-' . Infliximab is produced by a recombinant cell line cultured by continuous perfusion. Infliximab acts to neutralize the binding activity of TNFoc by inhibiting binding of TNF to its cell surface receptors. Serious side effects as a result of systemic intravenous infusions or injections have been reported with the use of infliximab, including fatal sepsis and serious infections.
- hypersensitivity symptoms include fever, rash, headache, sore throat, myalgias, polyarthraligias, hand and facial edema and/or dysphagia, anaphylaxis, convulsions, erythematous rash,
- Neurologic adverse events include optic neuritis, seizure and new onset or exacerbation and/or radiographic evidence of central nervous system demyeliiiating disorders, including multiple sclerosis.
- the formation of autoantibodies have also been observed, including symptoms suggestive of a lupus-like syndrome following treatment.
- Adalimumab is a recombinant human IgGl monoclonal antibody specific for human TlSF.
- Adalimumab was created using phage display technology resulting in an antibody with human derived heavy and light chain variable regions and human IgGl : ⁇ constant regions, and consists of 1330 amino acids with a molecular weight of approximately 148 kilodaltons.
- Adalimumab binds specifically to TNF- ⁇ and blocks its interaction with both the p55 and p75 TNF cell surface recepiors.
- Adalimumab also lyses TNF expressing cells in vitro in the presence of complement.
- Adalimumab does not bind or inactivate lymphotoxin (TNF- ⁇ ). Serious side effects from systemic administration have been reported with the intravenous administration or injection of adalimumab, including fatal sepsis and serious infections, including upper respiratory infections, bronchitis, urinary tract infections, pneumonia, septic arthritis, prosthetic and post-surgical infections, erysipelas cellulitis, diverticulitis, pyelonephritis, tuberculosis, and invasive oppoitunitistic infections caused by histoplasma, aspergillus and nocardia.
- adverse events included sinusitis, flu syndrome, nausea, abdominal pain, hypercholesterolemia, hyperlipidemia, hematuria, increased alkaline phosphatase levels, back pain, hypertension, as well as more infrequent serious adverse events, including pain, pelvic pain, thorax pain, arrthythmia, atrial fibrillation, cardiovascular disorder, congestive heart failure, coronary artery disorder, heart arrest, hypertensive encephalopathy, myocardial infact, palpitation, pericardial effusion, pericarditis, syncope, tachycardia, vascular disorders, and other disorders.
- Calcineurin inhibitors are a group of structurally diverse small molecule imraunomodulalors which function through the inhibition of calcineurin function.
- Calcineurin is a calcium-activated protein phosphatase which catalyses the dephosphorylation of cytoplasmic NFAT. Upon dephosphorylalion, NFAT migrates to the nucleus and forms a regulatory complex involved in the transcription of cytokines, such as TNF- ⁇ . IL -2. IL -3 and IL-4. Inhibition of calcineurin function blocks the dcphosphorylation event and subsequent cytokine transcription.
- calcineurin inhibition An unusual aspect of calcineurin inhibition is that cyclosporins, tacrolimus and pimecrolimus are required to form a complex with an immunophiJin for the inhibitory properties to be realized (Schreiber et ai, Immunol. Today (1992), 13:136-42; Liu et al. Cell (1991), 66:807-15).
- the immunophilin is cyclophilin; tacrolimus and pimecrolimus. bind to the FK506-binding protein (FKBP).
- Cyclosporine is an 1 1 -residue cyclic peptide produced as a metabolite of the fungus
- Beauvena nivea has the chemical name cyciof[(E)-(2S,3R,4R)-3-hydroxy-4-methyl-2- (methylamino)-6-octenoyl]-L-2-aminobutyryl-N-methylglycyl-N-methyl-L-leucyl-l..-valyl-N- methyl-l ⁇ leucyl-L-alanyl-D-alanyl-N-methyl-L-leucyl-N-raethyl-L-leucyl-N-methyl-L-valyi. It is provided in several formulations for both systemic or local administration.
- Sandimmune® provides cyclosporine in three different formulations: soft gelatin capsules, an oral solution or a formulation for injection.
- Sandimmune® is indicated for prevention of organ rejection in kidney, liver or heart transplants.
- Neoral® and Gengraf® provide cyclosporine in two formulations: soft gelatin capsules and an oral solution. They are indicated for prevention of organ rejection in kidney, liver or heart transplants, for treatment of patients with severe active, rheumatoid arthritis, or for treatment of severe psoriasis.
- Neoral® and Gengraf® provide increased bioavailability of cyclosporine.
- Restasis® provides cyclosporine in an ophthalmic emulsion formulation. It is indicated to increase tear production in patients with reduced tear production due to ocular inflammation associated with keratoconjunctivitis sicca.
- Tacrolimus also known as FK-506 or fujimycin, is a 23-membered macrolide natural product produced by Streptomyces tsukufraensis and has the chemical name [3S- [3R*[E(lS*,3S*,4S*)]. 4S*,5R*,8S*,9E,12R*,14R*,15S*,16R*,18S*,19S*,26aR*]]- 5,6.8,11, 12,13 ) 14 ) 15 x 16,17,18,19 ?
- the Prograf® formulation provides an oral capsule or a sterile solution for injection.
- Prograf® is indicated for prevention of organ rejection in liver, kidney or heart transplants.
- the Protopic® formulation is indicated for the treatment of moderate-to- severe atopic dermatitis.
- PimecroMmus is a semi-synthetic analog of tacrolimus and has the chemical name
- tacrolimus and piniccrolimus do not suppress Langerhans' cells or dermal connective tissue and therefore do not cause atrophy of the skin, unlike corticosteroids (Stuetz et al, Int. Arch. Allergy Immunol. (2006), 141 :199-212: Queille-Roussel et al, Br. J.
- the auris-acceptable controlled release immunoinodulating formulation comprises a calcineurin inhibitor. In another embodiment, the auris-acceptable controlled release immunomodulating formulation comprises cyclosporine. In another embodiment, the auris- acceptable controlled release immunomodulating formulation comprises tacrolimus. In another embodiment, the auris-acceptable controlled release immunomodulating form ⁇ lalion comprises pimecrolimus. In. another embodiment, the auris-acceptable controlled release imrn ⁇ nomodulatitig formulation comprises a calcineurin inhibitor which induces toxicity upon systemic administration. ⁇ 00278
- immunomodulating- ⁇ agents for the treatment of autoimmune and/or inflammatory disorders include other agents that have been used to treat autoimmune and inflammatory disorders, including corticosteroids, local anesthetic agents, chemotherapeutic agents, including Cytoxan, azathiaprine or methotrexate; treatment with collagen, gamma globulin, interferons, Copaxone, or combinations thereof. Accordingly, also contemplated within the scope of the embodiments herein is the use of other pharmaceutical agents in combination with the imraunomodulating compositions and formulations disclosed in the treatment of autoimmune otic disorders. In addition, other agents that have been used to treat autoimmune and inflammatory disorders, including corticosteroids, local anesthetic agents, chemotherapeutic agents, including Cytoxan, azathiaprine or methotrexate; treatment with collagen, gamma globulin, interferons, Copaxone, or combinations thereof. Accordingly, also contemplated within the scope of the embodiments herein is the use
- pharmaceutical agents are optionally used to treat attendant symptoms of AIED or other autoimmune disorder, including vomiting, dizziness and general malaise.
- NF-KB is in the cytoplasm as part of a protein complex with the protein inhibitor of JNF-KB, also known as IKB.
- Activation of NF-KB depends on phosphorylation-induced ubiquitination of the IKB.
- the TKB undergoes a rapid degradation through the 26S proteasome and the free NF-icB migrates to the nucleus to activate pro-inflammatory gene transcription.
- the phosphorylation event which releases NF- ⁇ B is mediated by the IKB kinase (IKK) complex, composed of IKK kinases.
- IKK IKB kinase
- IKK- ⁇ and IKK- ⁇ Two IKK enzymes, generally referred to as IKK- ⁇ and IKK- ⁇ (Woronicz et al. Science (1997), 278:866; Zandi et al. Cell (1997). 91 :243) or IKK-I and IKK-2 (Mercurio et al. Science (1997), 278:860) have been discovered. Both forms of IKK can exkst as homodiraers and as ⁇ KK- ⁇ /lKK- ⁇ heterodimers.
- Another component of the IKB kinase complex is a regulatory protein, known as lKK- ⁇ or NEMO (NF- ⁇ B-Essential Modulator) (Rothwarf et al. Nature (1998), 395:297).
- NEMO does not contain a catalytic domain, and thus it appears to have no direct kinase activity and it probably serves a regulatory function.
- IKK- ⁇ /TKK- ⁇ heterodimer associated with either a dimer or a trimer of NEMO (Rothwarf et al. Nature (1998) 395:297)
- Biochemical and molecular biology' experiments have identified IKK- ⁇ and IKK- ⁇ as the most likely mediators of TNF-oc-induced IKB
- IKK- ⁇ inhibitors have been identified. SPC-839 has been extensively studied. It inhibits IKK- ⁇ with an ICs () of 62 nM and reduces paw edema in a rat arthritis model at 30 rag/kg. Carboline PS-1 145 inhibits the IKK complex with an IC 5 ⁇ of 150 nM and reduces the production of TNF- ⁇ in LPS-chatlenged mice. BMS-345541, an allosteric inhibitor, inhibits IKK- ⁇ with an IC 5 O of 0.3 ⁇ M. In the mouse collagen-induced arthritis model it significantly reduced the severity of disease at a 30mg/kg dose. A scientific review of IKK inhibitors has been published (Karin ct «/., Nature Reviews Drug Discovery (2004), 3, 17-26), incorporated herein by reference for such disclosure.
- the auris-acceptable controlled release iramunomod ⁇ lating formulation comprises an IKK inhibitor.
- the auris-acceptable controlled release imraunomodulaiing formulation comprises a IKK- ⁇ inhibitor.
- the auris- acceptable controlled release immunomoduiating formulation comprises a IKK inhibitor which induces toxicity upon systemic administratiori.
- the auris-acceptable controlled release immunomoduiating formulation comprises a IKiC inhibitor which is not orally absorbed.
- the auris-aeceptabie controlled release immunomoduiating formulation comprises an IKK inhibitor selected from SPC-839, PS-Il 45, BMS-345541, or SC-514.
- the auris-acceptable controlled release immunomoduiating formulation comprises an IKK inhibitor selected from compounds disclosed in the following group of patent publications: WOl 99901441, WO2001068648. WO200206G386, WO2002030353, WO2003029242, WO2003010163, WO2001058890, WO2002044153, WO2002024679,
- lnterleukins are a class of cytokines. In certain instances, they are signaling molecules secreted by leukocytes having encountered a pathogen. In certain instances, the secretion of interleukins activates and recruits additional leukocytes to the site of infection. Iu certain instances, the recruitment of additional leukocytes to the site of infection results in inflammation (due to the increase in leukocyte containing lymph).
- IL-I ⁇ , IL-I ⁇ , IL-2, and IL-8 are found in middle ear effusions. In certain instances, IL-l ⁇ and IL-I ⁇ are also found in the epithelium of cholesteatomas.
- ⁇ l-1 is a class of interleukins comprised of IL-i ⁇ , and IL-l ⁇ .
- IL-I is made by macrophages, B cells, monocytes, and dendritic cells (DC).
- DC dendritic cells
- U binds to receptors U.lRl/CD121a and ⁇ LlR2/CD121b.
- the binding of IL-I to its receptors results in an increase in cell-surface adhesion factors. This enables the migration of leukocytes to the site of infection.
- IL-2 is made by TH-I cells and binds to the receptors CD25/TL2Ra, CDl 22IL2Rb, and CD132/lL2Rg. 11-2 secretion is stimulated by the binding of an antigen to a TTM cell. The binding of IL-2 to a receptor stimulates the growth, and differentiation of memory T cells.
- IL-S is made by macrophages, lymphocytes, epithelial cells, and endothelial cells. It binds to CXCRl/ ⁇ L8Ra and CXCR2/IL8Ra/CD128. Secretion of IL-8 initiates neutrophil chemotaxis to the site of infection.
- a subject in need thereof is administered an inhibitor of a pro ⁇ inflammatory interleukin.
- the pro-inflammatory interleukin is IL- 1 ⁇ , IL-I ⁇ . IL-2, or 1L-8.
- the inhibitor of a pro-inflammatory interleukin is a WS-4 (an antibody against IL-8); [Ser IL-S] 72 ; or [Ala IL-8j ⁇ ? (See U.S. Patent No.
- Platelet activating factor antagonists are contemplated for use in combination with the immunomodulating formulations disclosed herein.
- Platelet activating factor antagonists include, by way of example only, kadsurenone, phomactin G 1 ginsenosides.
- TNF- a Converting Enzyme (TACE) Inhibitors [00288] TNF- ⁇ is initially expressed on the cell surface as a 26 kDa, 233-a ⁇ nirio acid, membrane- bound precursor protein. Proteolytic cleavage of the membrane-bound TNF- ⁇ by lite matrix inetalloproteinase TNF- ⁇ converting enzyme occurs between Ala-76 and Val-77 and results in a 17 kDa mature TNF- ⁇ which exists as a soluble ti ⁇ mer. Inhibition of the proteolytic cleavage could provide an alternative to the use of protein-based therapeutics in antiinflammatory therapy.
- TACE is thought to be involved in the processing of other proteins in addition to TNF- ⁇ .
- TACK inhibition indicates that TACE also acts on other membrane bound proteins, such as TNl 5 RI and TNFRII.
- Inhibitor OW3333 has a TACE IC 50 of 40 nM and an IC ⁇ 0 of 0.97 ⁇ M for inhibiting TNF- ⁇ production in the LPS-induced human PBMC cells (Conway et al, J. Pharmacol. Exp. Ther. (2001), 298:900).
- Nitroarginine analog A has an ICn, TACE ICs 0 of 4 nM and an IC 50 of 0.034 ⁇ M for inhibiting TNF- ⁇ production in the LPS-induced MonoMac-6 cells (Musso et al, Bioorg. Med. Chem. Lett.
- the auris-acceptable controlled release anii-TNF formulation comprises a TACE inhibitor.
- the auris-acccptabie controlled release anti-TNF formulation comprises a TACE inhibitor which induces toxicity upon systemic administration.
- the auris-acceptable controlled release anti-TNF formulation comprise a TACE inhibitor which is not orally absorbed.
- the auris-acceptable controlled release anti-TNF formulation comprises a TACH inhibitor selected from Nitroarginine analog A, GW3333, TMI-I, BMS-561392, DPC-3333, TMJ-2, BMS-566394, TMI- 005, apratastau GW4459.
- Toll-like Receptor Inhibitors selected from Nitroarginine analog A, GW3333, TMI-I, BMS-561392, DPC-3333, TMJ-2, BMS-566394, TMI- 005, apratastau GW4459.
- Toll-like receptors are a family of at least 12 pattern recognition cell-surface and intracellular receptors. The family is defined by the presence of two domains: a ligand-binding domain with multiple leucine-rich repeats, and a short Toll/11- 1 receptor domain; the latter controlling the initiation of downstream-signaling cascades. Ia certain instances, the receptors are activated by the binding of structurally conserved molecules (i.e. the "patterns") found on pathogens. Hach receptor recognizes and binds to specific conserved molecules found on pathogens (e.g. TLR2 - lipopeplides; TLR3- viral dsRNA; TLR4 LPS; TLR5 ...
- TLR2 - lipopeplides e.g. TLR2 - lipopeplides; TLR3- viral dsRNA; TLR4 LPS; TLR5 ...
- TLR.9 CpG DNA ilagellm; TLR.9 CpG DNA.
- TLR2 a ⁇ d/or TLR4 is up- regulated upon exposure to nontypeable Hemophilus influenzae (NTHi). Infection by NTHi is a common cause of otitis media.
- Toll-like receptors belong to a class of single membrane-spanning non-catalytic receptors that recognize structurally conserved molecules derived from breached microbes are believed to play a key role in the innate immune system. Toll-like receptors thus recognize molecules that are broadly shared by pathogens, but are distinguishable from the host molecules. These receptors form a superfamily with Interleukin-1 receptors, and have in common a Toll-like receptor domain. Toll- like receptor agonists, such as CQ-07001 , can stimulate Toll-like receptor 3 function, triggering anti- inflammatory and tissue regeneration activity.
- Toll-like receptor modulators thus, have implication for use in both auris interna disorders, including AIED, and auris media diseases, including otitis media.
- toll-like receptor modulators include toll-like receptor antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- Other toll-like receptor modulators include but are not limited to
- poly(I:C) polyinosmie-p ⁇ lycytidylie acid
- poly AU other nucleic acid molecules, including dsRNA agonists (such as AMPLIGEN®, Hemispherx, Inc., Rockville MD; and POLYADENUR&, Ipsen), and are also contemplated within the scope of the embodiments disclosed herein.
- dsRNA agonists such as AMPLIGEN®, Hemispherx, Inc., Rockville MD; and POLYADENUR&, Ipsen
- the TLR inhibitor is an ST2 antibody; sST2-Fc (functional murine soluble ST2-human IgGl Fc fusion protein; see Biochemical and Biophysical Research
- PD98059 (2-(2-ammo-3-methoxyphenyl)-4H-1-Benzopyran-4-one); chloroquine; and an immune regulatory oligonucleotide (for disclosures relating to IROs see U.S. Patent ApplicationPublication No. 2008/0089883),
- agents which reduce or ameliorate symptoms or effects as a result of autoimmune disease including autoimmune inner ear disease (AIED).
- some embodiments may incorporate the use of agents which block the effects of TNF-OC, including but not limited to anti-TNF agents.
- anti- TNF agents include etanercept (ENBREUD), infliximab (REMICADE®) and adalimumab
- HUMIRA ⁇ chemotherapeutic agents
- Other pharmaceutical agents to treat autoimmune disorders include chemotherapeutic agents, including Cytoxan, azathiaprine or methotrexate; treatment with collagen, gamma globulin, interferons. Copaxone, or combinations thereof.
- Interleukin-1 is a pleiotropic cytokine that plays a role in the modulation of local as well as systemic inflammation, immune regulation and hemopoiesis.
- IL-I ⁇ a member of the IL-I family, has been implicated in angiogenesis processes, including tumor angiogenesis.
- TL-I has been shown to stimulate the synthesis of inflammatory eicosanoids in macrophages, fibroblasts, synovial cells and chondrocytes, and is believed to contribute to leukocyte activation and tissue destruction in arthritic models.
- IL-I modulators include an IL-I antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- IL-I modulators include but are not limited to antibodies that specifically recognize IL-I subunits or its receptors, proteins, peptides, nucleic acids, and small molecule therapeutics.
- ILL-I modulators are TI-- 1 antagonists, including, for example, AF12198, IL-I natural antagonists, inactive receptor fragments that bind to IL-I molecule, and antisense molecules or factors that block expression of IL-I cytokine proteins.
- TI-- 1 antagonists including, for example, AF12198, IL-I natural antagonists, inactive receptor fragments that bind to IL-I molecule, and antisense molecules or factors that block expression of IL-I cytokine proteins.
- IL-I antagonists are IL-I antibodies including, by way of example, anafcinra
- modulators of IL-I are antibodies that modulate cytokines and/or growth factors that affect the release and/or expression of IL-I, including, by way of example, ranibizurnab, tefibazumab, and bevacizuraab.
- IL-I modulators are IL-I traps that attach to IL-I and neutralize IL-I before it can bind to cell surface receptors and include, but are not limited to, riloiiocept (Arcalyst®).
- RNA interference are utilized.
- the agent that inhibits or down-regulates the target is an siRNA molecule.
- the sfRNA molecule inhibits the transcription of a target by RNA interference (RMAi).
- RMAi RNA interference
- dsRNA double stranded RNA
- a 20-25 bp siRNA molecule with sequences complementary to a target is generated.
- the 20-25 bp siRNA molecule has 2-5 bp overhangs on the 3' end of each strand, and a 5' phosphate terminus and a 3' hydroxy! terminus. In some embodiments, the 20-25 bp siRNA molecule has blunt ends.
- Molecular Cloning A Laboratory Manual, second edition (Sambrook et al., 1989) and Molecular Cloning: A Laboratory Manual, third edition (Sambrook and Russel, 2001), jointly referred to herein as "Sambrook”); Current Protocols in Molecular Biology (F. M. Ausubel et al., eds., 1987, including supplements through 2001); Current Protocols in Nucleic Acid Chemistry John Wiley & Sons, Inc., New York, 2000) which are hereby incorporated by reference for such disclosure.
- the dsRNA or siRNA molecule is incorporated into a controlled- release auris-acceptable microsphere or microparticle, hydrogei. liposome, actinic radiation curable gel, solvent-release gel, xerogel, paint, foam, in situ forming spongy material, or thermoreversible gel.
- the auris-acceptable microsphere, hydrogei, liposome, paint, foam, in situ forming spongy material, nanoeapsuie or nanosphere or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere or microparticle, actinic radiation curable gel, solvent-release gel, hydrogei, liposome, or thermoreversible gel is injected through the round window membrane.
- the auris-acceptable microsphere, hydrogei, liposome, paint, foam, in situ forming spongy material, actinic radiation curable gel, solvent-release gel, nanoeapsuie or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination thereof.
- dsRN A or siRNA molecule after administration of the dsRN A or siRNA molecule, cells at the site of administration (e.g. the cells of cochlea, Organ of Corti, and/or the vestibular labyrinth) are transformed with the dsRNA or siRNA molecule.
- the dsRNA molecule is cleaved into multiple fragments of about 20-25 bp to yield siRNA molecules.
- the fragments have about 2bp overhangs on the 3' end of each strand.
- an siRNA molecule is divided into two strands (the guide strand and the anti-guide strand) by an RNA-induced Silencing Complex (RISC).
- RISC RNA-induced Silencing Complex
- the guide strand is incorporated into the catalytic component of the RISC (i.e. argonaute).
- the guide strand binds to a complementary target mRNA sequence.
- the RJSC cleaves the target mRNA.
- the expression of the target gene is down-regulafed.
- a sequence complementary to a target is ligated into a vector.
- the sequence is placed between two promoters.
- the promoters are orientated in opposite directions.
- the vector is contacted with a cell.
- a cell is transformed with the vector.
- sense and anti-sense strands of the sequence are generated,
- the sense and anti-sense strands hybridize to form a dsRNA molecule which is cleaved into siRNA molecules.
- the strands hybridize to form an siRNA molecule.
- the vector is a plasmid (e.g pSUPER; pSUPER.neo; pSlJPER.neo+gfp).
- the vector is incorporated into a control led-release auris-acceplable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel.
- the aims-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere or microparticle, hydrogel. liposome, or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination (hereof. Aural Pressure Modulators
- Contemplated for use with the formulations disclosed herein are agents that treat disorders of the auris, and/or modulate the cells and structures of the aiiris.
- an aquaporin is involved in fluid homeostasis.
- AQP2 mRNA is elevated in rats treated with vasopressin above the levels observed in control animals.
- Aquaporin-1 is expressed in the cochlea and endolymphatic sac.
- Aquaporin-1 is expressed in the spiral ligament, the Organ of Corti, the scala tyr ⁇ pani, and the endolymphatic sac.
- Aquaporin-3 is expressed in the stria vascularis, the spiral ligament, the Organ of Corti, the spiral ganglion and the endolymphatic sac.
- aquaporin 2 (AQP2) mRNA is elevated above normal levels in individuals with endolymphatic hydrops.
- the aquaporin is aquaporin 1, aquaporin 2 and/or aquaporin 3.
- the agent that modulates an aquaporin e.g. aquaporin 1 , aquaporin 2 or aquaporin 3
- the aquaporin antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist includes, but is not limited to, substance P; RU-486; tetraethylammonium (TEA); an aati-aquaporin antibody; a vasopressin and/or a vasopressin receptor antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, ailosteric antagonist, and/or orthosteric antagonist; or combinations thereof.
- Estrogen-related receptor beta (ERR-beta; also known as Nr3b2), an orphan nuclear receptor, is specifically expressed in and controls the development of the endolymph-producing cells of the innter ear: the strial marginal cells in the cochlea and the vestibular dark cells in the ampulla and utricle. (Chen et al. Dev. Cell. (2007) 13:325-337). Nr3b2 expression has been localized in the endoiymph-secreting strial marginal cells and vestibular dark cells of the cochlea aud vestibular apparatus, respectively.
- ERR/Nr3b2 Treatment with antagonists to ERR/Nr3b2 may assist in reducing endolymphatic volume, and thus alter pressure in the auris interna structures. Accordingly, agents which antagonize ERR/Nr3b2 expression, protein production or protein function are contemplated as useful with the formulations disclosed herein.
- Gap junctions are intracellular connections.
- a gap junction connects the cytoplasm of two cells.
- a gap junction facilitates the passage of small molecules (e.g. IP-O and ions between the cells.
- gap junctions are formed of connexins (e.g. six connexins form a connexon and two connexons form a gap junction). There are multiple connexins (e.g.
- Cx23, Cx25 « Cx26, Cx29, Cx30, Cx30.2, CxSO.3, Cx3U Cx31.1, Cx31.9.
- Cx26 and Cx43 are expressed in a spiral limbus, a spiral ligament, a stria vascularis, cells of the Organ of Corti.
- non-syndromic deafness is associated with mutations in genes (e.g. GJB2) encoding connexins (e.g.
- Cx26 Jn certain instances, sensorineural hearing loss is associated with mutations in genes encoding connexins (e.g. Cx26). fa certain instances, the expression of Cx26 and Cx43 is upregulated in a cholesteatoma. In certain instances, the expression of Cx26 is upregulated following acoustic trauma. In certain instances, gap junctions facilitate the movement of 1C 1 ions in endolymph. [00307 ⁇ Accordingly, some embodiments disclosed herein incorporate the use of agents that modulate gap junction proteins. In some embodiments, the gap junction protein is a connexin.
- the agent that modulates a connexin is a connexin agonist, partial agonist, and/or positive allosteric modulator of a connexin.
- the connexin agonist, partial agonist, and/or positive alioste ⁇ c modulator includes, but is not limited to, astaxanthin; rotigaptide; adenosine; corticotropin-releasing hormone; or combinations thereof,
- Vasopressin is a hormone that plays an important part in circulatory and water homoeostasis. This hormone is synthesised by neurosecretory cells located predominantly in two specific hypothalamic nuclei—the supraoptic nucleus and the paraventricular nucleus. These neurons have axons that terminate in the neural lobe of the posterior pituitary gland
- vasopressin receptor subtypes (neurohypophysis) in which they release vasopressin.
- the three vasopressin receptor subtypes (VPIa, VPIb and VP2) all belong to the G-protein coupled receptor family and have differing tissue distributions.
- the VPIa receptor is predominantly located in the vascular smooth muscle, hepatocytes and blood platelets.
- the VPIb receptors are found in the anterior pituitary.
- 'Hie VP2 receptors are localized in the collecting duct of the kidney and regulate the presentation of aquaporin-2 channels at the apical cell surface. The effect of modulation of the VP2 subtype provides readily observed changes in urine volume and electrolyte levels to determine the pharmacological effects of anti-diuresis.
- Vasopressin regulates systemic osmolality by controlling urinary volume and composition.
- Vasopressin is secreted in response to increases in plasma tonicity (very sensitive stimulus) or to decreases in plasma volume (less sensitive stimulus).
- Vasopressin mainly regulates urinary volume by binding to the VP receptor in the collecting duct of the kidney.
- the VP receptor also exists in the inner ear of rodents, and aquaporin-2 (AQP2), a VP mediated water channel protein, is also expressed (Kitano etal. Ne ⁇ roreport (1997), 8:2289-92). Water homeostasis of the inner ear fluid was confirmed to be regulated using the VP-AQP2 system (Takeda et aJ.
- VP Contemplated for use with the formulations disclosed herein are agents that treat disorders of the auris, and/or modulate the cells (e.g., auris sensory cells) and structures of the auris.
- VP is involved in fi ⁇ id homeostasis.
- VP is involved in endolymph and/or perilymph homeostasis.
- an increase in endolymph volume increases pressure in the vestibular and cochlear structures.
- plasma levels of VP are elevated above normal levels in endolymphatic hydrops and/or Meniere's Disease.
- Vasopressin receptor modulators can be differentiated based upon their efficacy relative to the vasopressin peptide hormone.
- a vasopressin receptor full agonist is a mimic of the native peptide.
- a vasopressin receptor antagonist blocks the effect of the native peptide.
- a partial agonist can serve as a mimic of the native peptide and induce a partial response, or in the presence of elevated levels of the native peptide, a partial agonist competes with the native peptide for receptor occupancy and provides a reduction in efficacy, relative to the native peptide alone.
- an inverse agonist serves to reverse the activity of the receptor.
- some embodiments incorporate the use of agents that modulate vasopressin and/or a vasopressin receptor.
- the agent that modulates vasopressin and/or a vasopressin receptor is a vasopressin and/or a vasopressin receptor antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- the vasopressin and/or a vasopressin receptor antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, aUosteric antagonist, and/or orthosteric antagonist includes, but is not limited to, an anti-vasopressin antibody; an anti-vasopressin receptor antibody; lithium; OPC-31260 (( ⁇ )-5-dimethylamino-l-(4- [2-metliylbenzoyIamiuo]benzoyl)- 2,3,4,5-tetrahydr ⁇ - 1 H-benzajsepm hydrochloride); WAY-140288 (N-[4-[3- (Dimethylaminomethyl)-lO,! ?
- vasopressin antagonists are contemplated as useful with (he formulations disclosed herein.
- vasopressin antagonists include, but are not limited to OPC-31260, WAY- 140288, CL-385004, lolvaptan, conivaptan, SR 121463A, VPA 985, Valium (diazepam), benzodiazepines and combinations thereof.
- Testing of vasopressin antagonists may include testing and calculating hydrops reduction with treatment in a guinea pig animal model. See, e.g. , Chi et al. "The quantification of endolymphatic hydrops in an experimental animal model with guinea pigs", J. Oto-Rhino-Larynol. (2004) 66:56-61.
- Agonists of the VP2 receptor are known, including OPC-51803 and related analogs (Kondo et al., ). Med. Chem. (2000) 43:4388; Nakamura et al., Br. J. Pharmacol. (2000) 129(8): 1700;
- Antagonists of the VP2 receptor include lixivaptan, tolvaptan, conivaptan, SR-121463 and OPC-31260 (Martin et al., J. Am. Soc. Nephrol. (1999) 10(10):2165; Gross et al., Exp. Physiol. (2000) 85: Spec No 253S; Wong et al., Gastroent April 2000, vol 118, 4 Suppl. 2, Part 1 ); Norman et al. ? Drugs Fut.
- the over-activation of the NMDA glutamate receptors by the binding of excessive amounts of glutamate results in the excessive opening of the ion channels under their control. In certain instances, this results in abnormally high levels of Ca 2 ' and Na ' entering the neuron.
- the influx of Ca 2+ and Na ⁇ into the neuron activates multiple enzymes including, but not limited to, phospholipases, endonucleases, and proteases.
- the over-activation of these enzymes results in tinnitus, and'or damage to the cytoskeleton, plasma membrane, mitochondria, and DNA of the neuron.
- the NMDA receptor modulator neramexane treats, and/or ameliorates the symptoms of tinnitus.
- the agent that modulates the NMDA receptor is an NMDA receptor antagonist.
- the agent that modulates an NMDA receptor is an NMDA receptor antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- the agent which antagonizes the NMDA receptor includes, but is not limited to, 1-aminoadamantane, dextromethorphan, dextrorphan, ibogatne, ketamine, nitrous oxide, phen.cyclid.ine, riluzole, tilet ⁇ mine, memantine, neramexane, dkocilpine, aptiganel, remaciraide, 7-chloroJkynurenate, DCKA (5,7-dichlorokymtreiuc acid), kynurenic acid, 1-aminocyciopropanecarboxyUc acid (ACPC).
- 1-aminoadamantane dextromethorphan
- dextrorphan ibogatne
- ketamine nitrous oxide
- phen.cyclid.ine riluzole
- tilet ⁇ mine memantine, neramexane, dkocilpin
- AP7 (2-amino-7- phosphonoheptanoic acid), APV (R-2-ammo-5-phosphonopentanoate), CPPene (3-[(R)-2- carboxypipera7in-4-yl]-prop-2-enyl-1-phosphomc acid); (+)-(lS, 2S)-1-(4-hydroxy-phenyJ)-2-(4- hydroxy-4 ⁇ pheriylpiperidino)-l -pro-panol; (I S.
- the epithelial sodium channel (RNaC. sodium channel non-neuronal 1 (SCNNl) or amiloride sensitive sodium channel (ASSC)) is a membrane-bound ion-channel that is permeable for Li -ions, protons and Na H -ions.
- the ENaC is located in the apical membrane of polarized epithelial cells and is involved in transepitheiial Na " -ion transport. Na7K+-ATPase is also involved in Na + transport and ion homeostasis.
- Modulators of the activity of ENaC modulate aural pressure and include, by way of example, the mineralcorticoid aldosterone, triamterene, and amiioride.
- compositions disclosed herein are agents which regulate aural pressure. Accordingly, some embodiments comprise osmotic diuretics.
- An osmotic diuretic is a substance that produces an osmotic gradient between two spaces. In certain instances, an osmotic diuretic produces an osmotic gradient between the endolymphatic and perilymphatic spaces. In certain instances, an osmotic gradient between the endolymphatic and perilymphatic spaces exerts a dehydrating effect on the endolymphatic space, tn certain instances, dehydrating the endolymphatic space decreases aural pressure.
- the aural pressure modulator is an osmotic diuretic.
- the osmotic diuretic is erythritol, raannitol, glucose, isosorbide, glycerol; urea; or combinations thereof.
- diuretic agents contemplated for use in combination with the aural pressure modulating formulations disclosed herein are diuretic agents.
- a diuretic agent is a drug that elevates the rate of urination.
- diuretics include triamterene, amiloride, bendroflumethiazide, hydrochlorotl ⁇ azide, furosemide, torsemide, bumetanide, acetazolamide, dorzolamide and combinations thereof.
- Progesterone Receptors include triamterene, amiloride, bendroflumethiazide, hydrochlorotl ⁇ azide, furosemide, torsemide, bumetanide, acetazolamide, dorzolamide and combinations thereof.
- Progesterone is a steroidal hormone.
- progesterone is a ligand for a progesterone receptor.
- progesterone is found in the brain.
- progesterone affects synaptic functioning.
- progesterone is associated with partial or complete loss of hearing. In certain instances, females taking progesterone and estrogen experienced greater hearing loss than females taking estrogen alone (e.g. about 10% to about 30%).
- some embodiments incorporate the use of agents that modulate progesterone and/or a progesterone receptor.
- the agent that modulates progesterone and/or a progesterone receptor is a progesterone and/or progesterone receptor antagonist, a partial agonist, an inverse agonist, a neutral or competitive antagonist, an allosteric antagonist, and/or an orthosteric antagonist.
- the agent that modulates progesterone and/or a progesterone receptor includes, but is not limited to, RU-486 ((I lb,17 b)-l I-[4-(Dimethylamino)phenyl]-17- hydroxy-l7-(l-propyn yl)-estra-4,9-dien-3-one); CDB-2914 ⁇ 17 ⁇ -acetoxy-l l ⁇ -[4-N,N- dimethylaininophenyl]-l 9-norpregna-4,9-diene-3,20-dione); CDB-4124 (i7 ⁇ -acetoxy-21 -raethoxy- U ⁇ -[4-N,N-dimethylamir) ⁇ pher)yl]-19-norpregna-4,9- diene-3,20-dione); CDB-4453 (17 ⁇ -acetoxy- 21-meth ⁇ xy-l 1 ⁇ -[4-N-methylaminophen
- ORG 33628 Organon
- onapristone ZK 98299
- asoprisnil ulipristal
- a anti-progesterone antibody an anti-progesterone receptor antibody; or combinations thereof.
- Prostaglandins are members of a group of fatty-acid derived compounds and depending upon the subtype, participate in a variety of functions, including control of constriction or dilation in vascular smooth muscle cells, aggregation or disaggregation of platelets, sensitization of spinal neurons to pain, increase or decrease in intraocular pressure, regulation of inflammatory mediation, regulation of calcium movement, control of hormone regulation and control of hormonal regulation.
- Prostaglandins have both paracrine and autocrine functions, and are a subclass of eicosanoid compounds.
- Prostaglandin analogues such as latanoprost, travoprost, unoprostone, minprostin F2 alpha and bimtoprost, have been shown in reduce intra-ocular pressure in glaucoma patients by enhancing the uveoscleral outflow, possibly through vasodilation mechanisms, in addition to effects on the trabecular meshwork.
- noise exposure induces 8- isoprostaglandin F2 ⁇ production in the cochlea, concomitant with an increase in vasoconstriction and reduced blood flow.
- prostaglandin analogue JB004/A improves hearing, and treats, and/or the symptoms of tinnitus and vertigo in patients suffering from M ⁇ niere's disease. Inhibition of prostaglandin F2 ⁇ function also reduces tinnitus in patients suffering from Meniere's disease, as well as improvements in hearing and vertigo. Finally, prostaglandins have been implicated in chronic inflammation associated with otitis media.
- one embodiment disclosed herein is the use of prostaglandin modulators, including latanoprost, travoprost, unoprostone. rnir ⁇ rostin F2-alpha, bimtoprost and SQ29548, and JB004/A (Synphora AB) to ameliorate or decrease inner ear and middle ear disorders, including Meniere's disease, tinnitus, vertigo, hearing loss and otitis media.
- prostaglandin modulators including latanoprost, travoprost, unoprostone.
- rnir ⁇ rostin F2-alpha, bimtoprost and SQ29548, and JB004/A Synphora AB
- ⁇ 00328 In some embodiments, where inhibition or down-regulation of a target is desired (e.g. genes
- RNA interference are utilized.
- the agent that inhibits or down-regulates the target is an siRNA molecule.
- the siRNA molecule is as described herein.
- immunomodulators and/or aural pressure modulators are useful in treatment of inflammatory otic disorders.
- any cytotoxic agent useful for the treatment of otic disorders e.g., inflammatory diseases of the ear or cancer of the ear, is suitable for use in the formulations and methods disclosed herein.
- the cytotoxic agent is an antimetabolite, an antifolate, an alkylating agent, a DNA intercalator, an anti-TNF agent, an anti-angiogenic agent, an anti-inflammatory agent, and/or an immunomodulatory agent.
- the cytotoxic agent is a protein, a peptide, an antibody, DNA, a carbohydrate, an inorganic molecule, or an organic molecule.
- the cytotoxic agents are cytotoxic small molecules.
- cytotoxic small molecules are of relatively low molecular weight, e.g., less than 1,000, or less than 600-700, or between 300-700 molecular weight. In some embodiments, the cytotoxic small molecules will also have anti-inflaminatory properties.
- the cytotoxic agents are methotrexate (RHEUMATREX®,
- Amethopterin cyclophosphamide
- THALIDOMID® thalidomide
- All of the compounds can be used to treat cancer, including cancer of the ear. Further, all of the compounds have anti-inflammatory properties and can be used in the formulations and compositions disclosed herein for the treatment of inflammatory' disorders of the ear, including AlED.
- cytotoxic agents are not without the potential for serious adverse side effects. Moreover, cytotoxic agents which demonstrate efficacy but are otherwise not approvable because of safety considerations is also contemplated within the embodiments disclosed herein.
- cytotoxic agents to the target otic structures for treatment of autoimmune and/or inflammatory disorders, as well as cancer of the ear, will result in the reduction or elimination of adverse side effects experienced with systemic treatment.
- localized treatment with the cytotoxic agents contemplated herein will also reduce the amount of agent needed for effective treatment of the targeled disorder due, for example, to increased retention of the active agents in the auris interna and/or media, to the existence of the biological blood barrier in the auris interna, or to the lack of sufficient systemic access to the auris media.
- cytotoxic agents used in the compositions, formulations, and methods disclosed herein are metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of cytotoxic agents, including methotrexate, cyclophosphamide, and thalidomide.
- Particularly preferred are metabolites, salts, polymorphs, prodatgs, analogues, and derivatives of cytotoxic agents, e.g., methotrexate, cyclophosphamide, and thalidomide, tl ⁇ t retain at least partially the cytotoxicity and anti-inflammatory properties of the parent compounds.
- analogues of thalidomide used in the formulations and compositions disclosed herein are lenalidomide
- Cyclophosphamide is a prodrug that undergoes in vivo metabolism when administered systemicaily.
- the oxidized metabolite 4-hydroxycyclophospliamide exists in equilibrium with aidophosphamide, and the two compounds serve as the transport forms of the active agent phosphoramide mustard and the degradation byproduct acrolein.
- preferred cyclophosphamide metabolites for incorporation into the formulations and compositions disclosed herein are 4-hydroxycyclophosphamide, aidophosphamide, phosphoramide mustard, and combinations thereof.
- cytotoxic agents used in the compositions, formulations, and methods disclosed herein, particularly for the treatment of cancer of the ear are any conventional cbemotherpeutic agents, including acridine carboxamide, actinomycin, lT-N-ailylammo- ⁇ -demethoxygeldanamycin, aminopterin, amsacrine, anthracycline, antineoplastic, antineopla&ton, 5-azaeytidine, azathioprine, BL22, bendamustine, biricodar, bleomycin, bortezomib, bryostafin, busulfan, caiycuiin, camptothecin, capecilabine, carboplatin, chlorambucil, cisplatin, cladribine, clofarabine, cytarabine, dacarbazine, dasatinib, daunorubicin, decitabine, dichloroacetic acid,
- proteasome inhibitors e.g., bortezomib
- raltitrexed rcbeccamycin
- mbitccan SN-38
- salinosporamide A satraplatin, streptozotoein, swainsonine, tariquidar, taxane, tegafur- ⁇ racil, ternozolomide, testolactone, thioTEPA, tioguanine, topotecan, trabectedin, tretinoin, tripiatin letranitrate, tris(2-chloroethyl)araine, troxacitabine, uracil mustard, valr ⁇ bicin, vinblastine, vincristine, vraorelbine, vonnostat, and ?.osuquidar.
- immunomodulalors and/or aural pressure modulators modulate the function of neurons and/or auris sensory cells.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris. promote the growth of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- some embodiments incorporate the use of agents which promote live survival of neurons and otic hair cells, and/or the growth of neurons and otic hair ceils.
- the agent which promotes the survival of otic hair cells is a growth factor.
- the growth factor modulator is a growth factor modulator antagonist, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner car. Accordingly, some embodiments incorporate the use of agents which rescue neurons and otic hair cells from cisplatin-induoed ototoxicity.
- Amilbstine also known as WR-2721, or ETH YOL®
- ETH YOL® is a cytoprotective agent. In certain instances, it prevents or ameliorates the damage to neuron and otic hair cells caused by cisplatin. In certain instances, doses at or above 40 mg/kg are needed to protect against or ameliorate the ototoxic effects of cisplatin.
- ICAM anti- intercellular adhesion molecule
- ICAM blocks the cascade of reactive oxygen species associated with exposure to noise.
- modulation of the cascade of reactive oxygen species associated with exposure to noise ameliorates or reduces the degeneration of neurons and/or hair cells of the auris.
- agents that are antibodies to ICAMs e.g., anti-IC ⁇ M-1 Ab, anti-ICAM-2 Ab or the like.
- Atohl is a transcription factor which binds to an E ⁇ box. In certain instances, it is expressed during the development of the hair cells of the vestibular and auditory systems. In certain instances, mice with Atohl knocked-out did no! develop otic hair ceils. In certain instances, adenoviruses expressing Atohl stimulate the growth and/or regeneration of otic hair cells in guinea pigs treated with ototoxic antibiotics. Accordingly, some embodiments incorporate modulation of the Atohl gene.
- a subject is administered a vector engineered to carry the human Atohl gene (the "Alohl vector").
- the Atohl vector is a retrovirus
- the Atohl vector is not a retrovirus (e.g. it is an adenovirus; a lentivirus; or a polymeric delivery system such as
- the Atohl vector is incorporated into a controlled-release auris- acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination thereof.
- the Atohl vector infects the cells at the site of administration (e.g. the ceils of cochlea. Organ of Corti, and/or the vestibular labyrinth).
- the Atohl sequence is incorporated into the subject's genome (e.g. when the Atohl vector is a retrovirus).
- the therapy will need to be periodically re-administered (e.g. when the Atohl vector is not a retrovirus).
- the therapy is re-administered annually.
- the therapy is re-administered semi-annually.
- the therapy is re-administered when the subject's hearing loss is moderate (i.e. the subject cannot consistently hear frequencies less than 41 db to SS dB) to profound (i.e. the subject cannot consistently hear frequencies less than 90 dB).
- a subject is administered the Atohl polypeptide.
- the Atohl polypeptide is incorporated into controlled-release auris-acceptable microsphere or microparticle, hydrogel, liposome, o ⁇ thermoreversible gel.
- the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel are examples of the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination thereof.
- the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel is placed in contact, with the round window membrane.
- a subject is administered a pharmaceutically acceptable agent which modulates the expression of the Atohl gene or activity of the Atohl polypeptide.
- the expression of the Atohl gene or activity of the Atohl polypeptide is up-regulated.
- the expression of the Atohl gene or activity of the Atohl polypeptide is down-regulated.
- a compound which agonizes or antagonizes Atohl is identified (e.g. by use of a high throughput screen).
- a construct is designed such lhat a reporter gene is placed downstream of an E-box sequence.
- the reporter gene is luciferase, CAT, GFP, ⁇ -lactamase or ⁇ -galactosidase.
- the Atohl polypeptide binds to the E-box sequence and initiates transcription and expression of the reporter gene.
- an agonist of Atohl aids or facilitates the binding of Atohl to the E-box sequence, thus increasing transcription and expression of the reporter gene relative to a pre-determined baseline expression level
- an antagonist, of Atohl blocks the binding of Atohl to the E- box, thus decreasing transcription and expression of the reporter gene relative to a pre-determined baseline expression level.
- BRN-3 is a group of transcription factors that include, but are not limited to, BRN-3a, B.RN-3b, and BRN ⁇ 3c. In certain instances, they are expressed in postmitotic hair cells. In certain instances, the hair cells of mice with BRN-3c knocked-out did not develop stereocilia and/or underwent apoptosis. In certain instances, BRN3 genes regulate the differentiation of inner ear supporting cells into inner ear sensory cells.
- a subject is administered a vector engineered to carry a human BRN- 3 gene (the ' ⁇ RN3 vector").
- the BRN3 vector is a retrovirus, In some embodiments, the BRN3 vector is not a retrovirus (e.g. it is an adenovirus; a lentivirus; or a polymeric delivery system such as METAFECTKNE®, SUPERFECT®, EFFECTENE®, or MlRUS' TRANSIT®).
- the subject is administered the BRN3 vector before, during, or after exposure to an ototoxic agent (e.g an aminoglycoside or cisplatin), or a sound of sufficient loudness to induce acoustic trauma.
- an ototoxic agent e.g an aminoglycoside or cisplatin
- a sound of sufficient loudness to induce acoustic trauma e.g an aminoglycoside or cisplatin
- the BRN3 vector is incorporated into a controlled-release auris- acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel is injected into the inner ear.
- the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination thereof.
- the BRN3 vector after administration of the BRN3 vector, the BRN3 vector infects the cells at the site of administration (e.g. the cells of cochlea, Organ of Corti, and/or the vestibular labyrinth).
- the BRN3 sequence is incorporated into the subject's genome (e.g. when the BRN3 vector is a retrovirus).
- the therapy will need to be periodically re-administered (e.g. when the BRN3 vector is not a retrovirus).
- a subject is administered a BRN3 polypeptide.
- the BRN3 polypeptide is incorporated into controlled-release auris-acceptabie microsphere or microparticle, hydrogel, liposome, or the ⁇ noreversible gel.
- the auris-acceptable microsphere, hydrogel liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or fhermoreversible gel is injected into the inner ear.
- the auris-aceepiable microsphere or microparticle, hydrogel, liposome, or thermoreversibie gel In some embodiments, the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, nanocapsule or nanosphere or thermoreversible gel is injected into the cochlea, the Organ of Corti, the vestibular labyrinth, or a combination thereof. In some embodiments, the auris-acceptable microsphere or microparticle, hydrogel, liposome, or thermoreversible gel. In some embodiments, the auris-acceptable microsphere, hydrogel, liposome, paint, foam, in situ forming spongy material, tianocapsule or nanosphere or thermoreversible gel is placed in contact with the round window membrane.
- a subject is administered a pharmaceutically acceptable agent which modulates the expression of the BRN3 gene or activity of the BRN3 polypeptide.
- the expression of the BRN3 gene or activity of the BRN3 polypeptide is up-regulated. In some embodiments, the expression of the BRN3 gene or activity of the BRN3 polypeptide is down-regulated.
- a compound which agonizes or antagonizes DRN3 is identified (e.g. by use of a high throughput screen).
- a construct is designed such that a reporter gene is placed downstream of a BRN3 binding site.
- the BRN3 binding site has the sequence ATGAATT AAT (SBNR3).
- the reporter gene is luciferase, CAT, GFP, ⁇ -lactamase or ⁇ -ga1actosidase.
- the BRN3 polypeptide binds to the SBNR3 sequence and initiates transcription and expression of the reporter gene.
- an agonist of BRN3 aids or facilitates the binding of BRN3 to the SBNR3 sequence, thus increasing transcription and expression of the reporter gene relative to a predetermined baseline expression level.
- an antagonist of BRN3 blocks the binding of BRN3 to the SBNR3, thus decreasing transcription and expression of the reporter gene relative to a pre-determined baseline expression level.
- I00355J Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- carbamate compounds protect neurons and otic hair cells from glutamate-induced excitotoxicity. Accordingly, some embodiments incorporate the use of carbamate compounds.
- the carbamate compounds are 2-phenyl-l ,2- ethanediol monocarbomates and diearbamates, derivatives thereof, and/or combinations thereof.
- the agent that promotes the survival of otic hair cells is an Estrogen Receptor agonist.
- the estrogen receptor agonist is a partial agonist or inverse agonist.
- Estrogen Receptor ⁇ is expressed in an outer hair cell, an inner hair cell, a spiral ganglion neuron, or combinations thereof.
- agonism of ERtt and/or ER ⁇ ameliorates hearing loss resulting from acoustic trauma.
- agonism of ERa and/or ER ⁇ increases and/or up-regulates the expression of a neurotroph gene and-'or the activity of a neurotroph polypeptide (e.g. BDNF).
- BDNF neurotroph polypeptide
- antagonism of ERa and/or ER ⁇ increases hearing loss resulting from acoustic trauma, hi certain embodiments, antagonism of ERa and/or ER ⁇ down-regulates the expression of a neurotroph gene and/or the activity of a neurotroph polypeptide (e.g. BDNF).
- a neurotroph polypeptide e.g. BDNF
- the ERa agonist is PPT (4,4',4"- ⁇ 4-Propy1 ⁇ P H] -pyrazole- 1,3,5- triyl)trisphenol): SKF-82958 (6-chloro-7,8-diliydroxy-3-allyl-1-phenyi-2,3 ⁇ 4,5-tctrahydro-1H-3- benzazepine); estrogen; estradiol: estradiol derivatives, including but not limited to 17- ⁇ estradiol, estrone, estrioL synthetic estrogen compositions or combinations thereof.
- the ER ⁇ agonist is ERpM 31 , phytoestrogen, MK 101 (bioNovo); VG-1010 (bioNovo); DPN
- estradiol derivatives including but not limited to 17- ⁇ estradiol, estrone, estriol, synthetic estrogen compositions or combinations thereof.
- Other ER ⁇ agonists include select benzopyrans and triazolo- tetrahydrofluorenones, disclosed in U.S. Patent No. 7,279,499, and Parker et al, Bioorg. & Med. Chem. Ltrs. 16: 4652-4656 (2006), each of which is incorporated herein by reference for such disclosure.
- a neurotroph is administered before, after, or simultaneously with an Estrogen Receptor ⁇ (ER ⁇ ) agonist.
- the neurotroph is BDNF, CNTF, GDNF. neurotrophin-3, iieurotrophin-4, and/or combinations thereof.
- fatty acids include but is not limited to an omega-3 fatty acid, an omega-6 fatty acid, or combinations thereof.
- the omega-3 fatty acid is ⁇ - Linol ⁇ nic acid, Stearidonic acid. Eicosatrienoic acid, Eicosatetraenoic acid, Eicosapeutaenoic acid, Docosapenlaenoic acid, Cl ⁇ panodonic acid, Docosahexaenoic acid, Tetracosapentaenoic acid, Tetracosahexaenoic acid (Nisinic acid), or combinations thereof.
- the omega- 3 fatty acid is ⁇ -Linolenic acid, docosahexaenoic acid, eicosapentaenoic acid, or combinations thereof, hi some embodiments, the omega-6 fatty acid is Linoleic acid.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear. Accordingly, some embodiments incorporate the use of agents which inhibit Notch 1 signaling.
- Notch 1 is a transmembrane polypeptide which participates in cell development.
- the agents which inhibit Notchl signaling are ⁇ -secretase inhibitors. In certain instances, the inhibition of Notch! by a ⁇ -secretase inhibitor, following treatment with an ototoxic agent, results in the production of otic hair cells.
- the ⁇ -secretase inhibitor is LY450139 (hydroxylvaleryl monobenzocaprolactam), L685458 (lS-ben2;yl-4R[l -[l-S-carbamoyl-2- phenethylcarbamoyl)-l S-3-methylbutylcarbamoyl]-2R-hydroxy-5-phenylpentyl ⁇ carbamic acid ten- butyl ester); LY411575 (N 2 -[(2S)-2-(3,5-difluorophenyl)-2-hydroxyethanoyl]-N'[(7S)-5-methyl-6- oxo-6,7-dihydro-5H-dibenzo[bid]azepin-7yrj-L-ala ⁇ iinamide), MK-0752 (Merck), tarenflurbil, and/or BMS-299897 (2-[(1R)-I -[[(4-ch)-2-[
- [00361 J Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear. Accordingly, some embodiments incorporate the use of agents which modulate glutamate receptors.
- the glutamate receptor is the AMPA receptor, the NMDA receptor, andOr a group II or 111 mGlu receptor.
- the agent that modulates the AMPA receptor is an ANtPA receptor antagonist.
- the agent which antagonizes the AMPA receptors is CNQX (6- cyano-7-nitroqumoxaline-2,3-dione); NBQX (2,3-dihydroxy-6-rntro-7-sulfamoyl- benzo[l]quinoxalme-2s3-dione); DNQX (6,7-dinitroquinoxaline-2.3-dione); kynurenic acid; 2,3- dihydroxy-6-nitro-7-s ⁇ ]famoylbenzo-[f
- the agent that modulates the NMDA receptor is an NMDA receptor antagonist.
- the agent which antagonizes the NMDA receptor is 1- aminoadamantane, dextromethorphan, dextrorphan, ibogaine, ketamine, nitrous oxide,
- the over-activation of the AMPA and NMDA glutamate receptors by the binding of excessive amounts of glutamate results in the excessive opening of the ion channels under their control. In certain instances, this results in abnormally high levels of Ca 2 " and Na- entering the neuron.
- the influx of Ca 2' and Na ' into the neuron activates multiple enzymes including, but not limited to, phospholipases, endonucleases. and proteases.
- the over-activation of these enzymes results in damage to the cytoskeleton, plasma membrane, mitochondria, and DNA of the neuron.
- the transcription of multiple pro-apoptotic genes and anti-apoptotic genes are controlled by Ca ⁇ + levels.
- the raGlu receptors unlike the AMPA and NMDA receptors, do not directly control an ion channel . However, in certain instances, they indirectly control the opening of ion channels by the activation of biochemical cascades.
- the mGlu receptors are divided into three groups. In certain instances, the members of groups 11 and ill reduce or inhibit post-synaptic potentials by preventing or decreasing the formation of cAMP. In certain instances, this causes a reduction in the release of neurotransmitters, especially glutamate.
- GRM7 is the gene which encodes the mGlu7 receptor, a group III receptor. In certain instances, the agonism of mGlu 7 results in a decrease in synaptic concentrations of glutamate. This ameliorates glutamate excitotoxicity.
- the glutamate receptor is a group II mGlu receptor.
- the agent which modulates the group II mGlu receptor is a group II mGlu receptor agonist.
- the group Ii mGlu receptor agonist is LY389795 ((-)-2-thia-4- aminobicyclo-hexane-4,6-dicarboxylate); LY379268 ((-)-2-oxa-4-aminobicyclo-hexane-4, ⁇ - dicarboxylale); LY354740 ((+)-2-aminobicyclo-hcxane-2,6dic ⁇ rboxylate); DCO-IV ((2S,2'R,3'R)-2- (2 ⁇ 3 !
- the mGlu receptor is a group III mGlu receptor.
- the group III mGlu receptor is mGlu7.
- the agent which modulates the group HI mGlu receptor is a group III mGlu receptor agonist.
- the group Hl mGlu receptor agonist is ACPT-I ((I S,3R,4S)-1 -aminocyclopentatie-1 ,3,4-tricarboxylic acid); L-AP4 ( j ⁇ +)-2-Amioo-4- ⁇ bosph ⁇ nobutyric acid); (S)-3,4-DCPG ((S)-3,4- dicarboxyphenylgiycine); (RS)-3,4-DCPG ((RS)-3 !
- RS-4- phosphonophenylglycine (RS)PPG): AMN082 (,N'-bis(diphenylmethyl)-l ,2-ethanediamine ⁇ hydrochloride); DCG-IV ((2S,2'R,3 1 R)-2-(2',3 ⁇ -dicarboxycyclopropyl)glyci.ne); and/or combinations thereof.
- the mGlu receptor is mGlu7.
- the agonist of mGlu7 is AMN082.
- the mGlu receptor modulator is 3,5- Dimethyl pyrrole-2.4-dicarboxylic acid 2-propyl ester 4-(! ,2,2-trimethyl-propyl) ester (3,5-dimethyI PPP); 3,3'-difluorobenzaldarine (DTO) 1 3,3'-dimlethoxybenzaldazine (DMeOB), 3,3'- dichlorobenzaldazine (IX 1 B) and other allosteric modulators of mGluR 5 disclosed in MoI. Pharmacol.
- DTO 3,3'-difluorobenzaldarine
- DMeOB 3,3'-dimlethoxybenzaldazine
- IX 1 B 3,3'- dichlorobenzaldazine
- a glutamate receptor modulator is a nootropic agent.
- Contemplated for use with the formulations disclosed herein are nootropic agents that modulate neuronal signalling by activating glutamate receptors.
- nootropic agents treat or ameliorate hearing loss (eg, N1HL) or tinnitus. Accordingly, some embodiments incorporate the use of nootropic agents including, and not limited to, piracetam, Oxiracetam, Aniracetam, Pramiracetam,
- Phenylpiracelam (Carphedon), Etiracetam, Levetiracetam, Nefiracetam, Nicoracetam, Rolziracetam, Nebracetam, Fasoracetam, Coluracetam, Dimiracetam, Brivaracetam, Seletracetam, and/or Rolipram for the treatment of N1HL or tinnitus.
- agents that modulate the degeneration of neurons and/or hair cells of the auris promote the survival and/or growth of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- some embodiments incorporate the use of agents which promote the survival of neurons and otic hair cells, and/or the growth of neurons and otic hair cells.
- the agent which promotes the survival of otic hair cells is a growth factor.
- the growth factor is a neurotroph.
- neurotrophs are growth factors which prevent cells from initiating apoptosis, repair damaged neurons and otic hair cells, and/or induce differentiation in progenitor cells.
- the neurotroph is brain-derived neurotrophic factor (BDNF), ciliary neurotrophic factor (CNTF), glial cell-line derived neurotrophic factor (GDNF), neurotrophin-3, neurotrophin-4, and/or combinations thereof
- the growth factor is a fibroblast growth factor (FGF), an insulin-like growth factor (IGF), an epidermal growth factor (EGF), a platlet-derived growth factor (PGF) and/or agonists thereof.
- the growth factor is an agonist of the fibroblast growth factor (FGF) receptor, the insulin-like growth factor ( ⁇ GF) receptor, the epidermal growth factor (EGF) receptor, and/or the platlet-derived growth tactor. In some embodiments, the growth factor is hepatocyte growth factor.
- FGF fibroblast growth factor
- ⁇ GF insulin-like growth factor
- EGF epidermal growth factor
- the growth factor is hepatocyte growth factor.
- the growth factor is an epidermal growth factor (EGF).
- EGF epidermal growth factor
- the EGF is heregulin (HR(J).
- HRG stimulates the proliferation of utricular sensory epithelium.
- HRG-bmdmg receptors are found in the vestibular and auditory sensory epithelium.
- the growth factor is an insulin-like growth factor (IGF).
- IGF insulin-like growth factor
- the IGF is IGF-I.
- the TGF-I is mecasermin.
- IGF-I attenuates the damage induced by exposure to an aminoglycoside.
- IGF-I stimulates the differentiation and/or maturation of cochlear ganglion cells.
- the FGF receptor agonist is FGF-2.
- the IGF receptor agonist is IGF-I . Both the FGF and IGF receptors are found in the cells comprising the utricle epithelium.
- the growth factor is hepatocyte growth factor (HGF).
- HGF hepatocyte growth factor
- EPO Erythropoietin
- G-CSF Grauuiocyte-colony stimulating factor
- GM-CSF Granulocyte- macrophage colony stimulating factor
- GDF9 Growth differentiation factor-9
- IGF Insulin- like growth factor
- GDF-8 Myostatin
- PDGF Platelet-derived growth factor
- TPO Thiombopoietin
- TGF- ⁇ Transforming growth factor alpha
- TGF- ⁇ Transforming growth factor beta
- VEGF Vascular endothelial growth factor
- the growth factor is a neurotropic
- neurotrophs are growth factors which prevent cells from initiating apoptosis, repair damaged neurons and otic hair cells, and/or induce differentiation in progenitor celis.
- the neurotropic is brain-derived neurotrophic factor (BDNF), ciliary neurotrophic factor (CNTF), glial cell-line derived neurotrophic factor (GDNF), neurotrophm-3, neurotrophin-4, and/or combinations thereof.
- the neurotropic is BDNF.
- BDNF is a neurotroph which promotes the survival of existing neurons (e.g. spiral ganglion neurons), and otic hair cells by repairing damaged cells, inhibiting the production of ROS, and inhibiting the induction of apoptosis. Iu certain embodiments, it also promotes the differentiation of neural and otic hair cell progenitors. Further, in certain embodiments, it protects the Cranial Nerve " VH from degeneration.
- BDNF is administered in conjunction with fibroblast growth tactor.
- the neurotroph is neurotropic n-3.
- neurotrophin-3 promotes the survival of existing neurons and otic hair cells, and promotes the differentiation of neural and otic hair cell progenitors. Further, in certain embodiments, it protects the VII nerve from degeneration.
- the neurotroph is CNTF, In certain embodiments, CNTF promotes the synthesis of neurotransmitters and the growth of neuritis. In some embodiments. CNTF is administered in conjunction with BDNF.
- the ne ⁇ rotroph is GDNF.
- GDNF expression is increased by treatment with ototoxic agents.
- cells treated with exogenous GDNF have higher survival rates after trauma then untreated cells.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- some embodiments incorporate the use of cells which participate in the repair of otic hair cells and neurons
- the cells which participate in the repair of otic hair cells and neurons are macrophages, microglia, and/or microglia-like cells.
- the concentration of macrophages and microglia increase in ears damaged by treatment with ototoxic agents.
- microglia-like cells eliminate waste from the Organ of Corti and participate in the structural repair of hair cells following treatment with the ototoxic antibiotic neomycin.
- agents that destroy neurons and/or otic hair cells are agents that destroy neurons and/or otic hair cells. Accordingly, some embodiments incorporate the use of agents which fatally damage and/or induce apoptosis. in the neurons and/or otic hair cells of the auris.
- the agents which fatally damage and/or induce apoptosis in the neurons and/or otic hair cells of the auris are the aminoglycoside antibiotics (e.g. gentamicin, and amikacin), the macrolide antibiotics (e.g erythromycin), the glyeopeptide antibiotics (e.g. vancomycin), the loop diuretics (e.g. furosemide) salicylic acid, and nicotine.
- agents that modulate the degeneration of neurons and/or hair cells of the auris Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, promote the growth of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, nialfunctioning, damaged, fragile or missing hairs in the inner ear. Further contemplated herein are agents that destroy neurons and/or otic hair cells. Accordingly, some embodiments incorporate the use of agents that modulate retinoblastoma protein (pRB). pRB is a member of the pocket protein family. It is encoded by the RBl gene.
- telomere shortening In certain instances, it inhibits transition from Gl to S phase by binding to and inactivating the E2f family of transcription factors. In certain instances, it also regulates differentiation, and survival of hair cells. In certain instances, pRB knock-out mice demonstrate increased prioliferation of hair cells.
- the agent that modulates one or more of the pRB is an agonist of pRB. In some embodiments, the agent that modulates one or more of the pRB is an antagonist of pRB. In certain instances, a compound which agonizes or antagonizes pRB is identified (e.g. by use of a high throughput screen).
- a construct is designed such that a reporter gene is placed downstream of an E2F binding sequence. In some embodiments, the binding sequence is TTTCGCGC. In some embodiments, the reporter gene is luciferase, CAT, GFP, ⁇ -!actamase or ⁇ - galactosidase. In certain instances.
- E2f binds to the binding sequence causing the transcription and expression of the reporter gene.
- an agonist of pRB causes an increase in the binding of pRB to E2f.
- the increase in binding of pRB and E2f results in a decrease in the transcription and expression of the reporter gene.
- an antagonist of pRB causes a decrease in the binding of pRB to E2f.
- the decrease in binding ofpRB and E2f results in a increase in the transcription; and expression of the reporter gene.
- the agent that modulates pRB is an siRNA molecule.
- the si RNA molecule is as described herein.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and/or hair cells of the auris, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear. Accordingly, some embodiments incorporate the use of salicylic acid. In certain instances, when administered before treatment with an aminoglycoside, it protects otic hair cells and spiral ganglion neurons from aminoglycoside ototoxicity.
- Contemplated for use with the formulations disclosed herein are agents that modulate the degeneration of neurons and hair cells, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs in the inner ear.
- excitotoxicity causes the excessive opening Of Na + channels. In certain instances, this results in excess Na " ions entering the neuron. In certain instances, the excess influx of Na H tons into the neuron causes the neuron to fire more often. In certain instances, this increased firing yields a rapid buildup of free radicals and inflammatory compounds. In certain instances, the free radicals damage the mitochondria, depleting the cell's energy stores.
- excess levels of Na ⁇ ions activate excess levels of enzymes including, but not limited to, phospholipases, endomicleases, and proteases. In certain instances, the over-activation of these enzymes results in damage to the cytoskeleton, plasma membrane, mitochondria, and DNA of the neuron. Accordingly, some embodiments incorporate the use of agents which antagonize the opening of Na" channels, in some embodiments, sodium channel blockers are as described herein.
- the agent is a stem cell
- tJhe agent is a partially or fully differentiated a ⁇ ris sensory cell.
- the differentiated auris sensory cell is derived from a human donor.
- the differentiated auris sensory cell is derived from a stem ceil, the differentiation of which was induced under artiflcia! (e.g. laboratory) conditions.
- Stem cells are cells that possess the capacity to differentiate into multiple cell types.
- Totipotent stem cells can differentiate into embryonic cells or extraembryonic cells. Pluripotent cells can differentiate into cells of any of endoderni, mesoderm, or ectoderm origin. Multipotent cells can differentiate into closely related cells (e.g hematopoietic stem cells). Unipotent cells can differentiate into only one type of cell, but like other stem cells have the characteristic of self- renewal.
- the stem cell is totipotent, pluripotent, multipotent, or unipotent. Further, stem cells can undergo mitotic division without themselves differentiating (i.e. se!f- renewai).
- Embryonic stem (ES) cells are stem cells derived from the epiblast tissue of the inner cell mass of a blastocyst or earlier stage embryo. ES cells are piuripotent. In some embodiments, the stem cell is an ES cell.
- Adult stem cells also known as somatic cells or germline cells
- Adult stem cells are pluripotent (for example, stem cells found in umbilical cord blood), miiltipotent or unipotent.
- the stem cell is an adult stem cell.
- a stem cell and/or a differentiated au ⁇ s sensory cell is administered in combination with a differentiation stimulating agent.
- the differentiation stimulating agent is a growth factor.
- the growth factor Fs a neur ⁇ trophin (e.g. nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3). neurotrophin-4 (NT-4), or novel neurotrophin-1 (NNTl).
- the growth factor is FGF, EGF, IGF, PGF, or combinations thereof.
- a stem cell and/or a differentiated auris sensory cell is administered to a subject in need thereof as a controlled release agent.
- a stem cell and/or a differentiated auris sensory cell is administered to a subject in need thereof as an immediate release agent (e.g. in a cell suspension) in combination with a controlled release auris sensory cell modulating agent.
- a controlled release auris sensory cell modulating agent is a vector comprising an Atohl or BRN3 gene, an siRNA sequence targeting RBl, a growth factor, or combinations thereof.
- a stem cell and/or a differentiated auris sensory cell is administered to the cochlea or vestibular labyrinth.
- a stem cell and/or a differentiated auris sensory cell is administered by via intratympanic injection, and/or a post-auricular incision.
- a stem cell and/or a differentiated auris sensory cell is contacted with the Organ of Corli, vestibulocochlear nerve, and/or crista ampuliaris.
- TH Thyroid Hormone
- TR ⁇ knock-out mice demonstrate a decreased responsiveness to auditory stimuli, and a decrease in K current in hair cells.
- the agent that modulates one or more of the TH receptors is an agonist of the one or more TH receptors.
- the agonist of one or more of the TH receptors is T,(3,5,3'-triiodo-L-thyroriine); KB-141 (3,5-dichloro-4-(4-hydroxy-3- isopropylphenoxy)phenylacetic acid); GC-I (3,5-dir0ethyl-4-(4'-hydroxy-3'-isopropylben7.yl)- phenoxy acetic acid); GC-24 (3,5-dimetliyl-4-(4'-hydroxy-3'-ben2yl)benzylphenoxyacetic acid); sobetirome (QRX-431); 4-OH-PCB106 (4 ⁇ )H-2 ⁇ 33 ⁇ 4 ⁇ 5'-pentachlorobiphenyl); MB07811 ((2R,4S)-4-(3
- TRPV Transient Receptor Potential Channel Vaniiloid
- TRPVl Transient Receptor Potential Channel Vaniiloid
- TRPV 1 following treatment with kanamycin, TRPV 1 is upregulated.
- antagonism of the TRPV 4 receptor makes mice vulnerable to acoustic trauma.
- capsaicin an agonist of TRPV 1, prevents hyperlocomotion following an ischemic event.
- the agent that modulates one or more of the TRPV receptors is an agonist of the one or more TRPV receptors.
- the agonist of one or more of the TRPV receptors is capsaicin, resiniferatoxi ⁇ . or combinations thereof.
- TRPV modulating include the TRPV modulators disclosed in US application publications 2005/0277643, 2005/0215572, 2006/0194801, 2006/0205773, 2006/0194801, 2008/0175794, 2008/0153857, 2008/0085901, 20080015183, 2006/0030618, 2005/0277646, 2005/0277631, 2005/0272931, 2005/0227986, 2005/0153984, 2006/0270682, 2006/0211741, 2006/0205980, and 2006/0100490, and/or combinations thereof.
- immunomodulators and/or aural pressure modulators modulate the function of neurons and/or a ⁇ ris sensory cells.
- Therapeutic agents which assist in restoring sensory hair cell presence or function are also contemplated herein. These therapeutic agents assist in the treatment of hearing loss In patients, including sensorineural hearing loss, presbycusis and hearing loss from excessive noise.
- IGF-I insulin-like growth factor 1
- IGF-I agonists or agents which upregulate the expression, production or function of IGF-I are optionally included with the formulations described herein.
- Adenosine is comprised of adenine attached to ⁇ bofuranose via a ⁇ -N9-glycosidic bond.
- adenosine is an inhibitory neurotransmitter. In certain instances, it functions as a iigand for four GPCRs - adenosine receptor Ai, adenosine receptor A 2A , adenosine receptor A 215 , and adenosine receptor Aj.
- the binding of adenosine to an adenosine receptor results ⁇ n (either partially or fully) an anti-inflammatory effect.
- the binding of adenosine to an adenosine receptor results in (either partially or fully) vasodialation. In certain instances, it is produced in response to cellular damage (e.g., hypoxia, and ischemia). For example, depolarization and asphyxia in the ear induce the release of adenosine into perilymph where it exerts a protective effect.
- cellular damage e.g., hypoxia, and ischemia
- ade ⁇ soine modulators are used in the treatment of cochlear and vestibular disorders.
- the adenosine modulator is ATTJ 13 (4-(3- (6-amino-9-(5-cyclopropylcarbmnoyl-3,4-d0iydroxytetrahydrofuran-2-yl)-9H-purin-2-yl)prop-2- ynyl)piperidine-1-carboxyhc acid methyl ester); GW328267X ((2R,3R,4S,5R)-2- ⁇ 6-amino-2-[(I - benzyi-2-hydroxyethyl)amino]-9H-purin-9-yl ⁇ -5-(2-ethyI-21I-te ⁇ -a ⁇ ol-5-yl)tetrahydr ⁇ .>furan-3,4- diol); CGS 21680 hydrochloride (4-f
- Atohl belongs to a family of basic Helix-Loop-Helix (b ⁇ ILH) genes that are involved in cell fate determination across phyla and systems, typically being expressed in proliferating precursors.
- b ⁇ ILH basic Helix-Loop-Helix
- Atohl m particular, is essential for hair cell differentiation, and plays a role as a differentiation factor of postmitotic hair cells. Studies have also shown that expression of Atohl , in combination with Bdnf t form afferent and efferent innervation in undifferentiated cells of epithelial origin.
- ATOH protein Treatment of with ATOH protein supports the role of Atohl in sensory hair cell development, inducing the formation of new sensory hair cells in cochlear structures, and restoring hearing and balance function.
- Gene therapy using vectors inserted with the Atohl ge ⁇ e further supports A ' T ' OH's role in promoting and maintaining sensory hair cell function.
- one embodiment disclosed herein is the use of ATOH proteins or manipulation oi ⁇ tohl expression to induce sensory hair cell development in hearing and balance disorders.
- a neurotrophic growth factor is administered to the auris interna via the formulations described herein to stimulate inner ear hair cell neurotrophic growth factors.
- the damage caused to spiral ganglion neurons removes not only neural activity, but also neurotrophin support that is normally supplied by hair cells, the absence of which leads to cell death via apopotosis.
- neurotrophic growth factor includes but is not limited to brain-derived neurotrophic fact, neurotrophin-3, gtial-derived neurotrophic factor, ne ⁇ rotrophm-4/5. nerve growth factor, ChIOrPhCOyItWo-CAA 1 IP (cptcAMP; a permeant cAMP analog), ciliary derived neurotrophic factor (CNTF) or combinations thereof.
- the sensory cell restorative agent is a brain-derived neutrophic factor (BDNF).
- the neurotrophic growth factor is ne ⁇ rotrophin-3 (NT-3).
- the neurotrophic growth factor is glial-derived neurotrophic factor (GDNF).
- the neurotrophic growth factor is a peptide or protein.
- the neurotrophic growth factor stimulates or enhances spiral ganglion neuron survival.
- KCNQ proteins form postassium channels, which play a role by preventing accumulation of potassium in hair cells. Potassium concentrations are high in the endolymph, giving the
- KCNQ function is correlated with outer hair cell (OHC) survival; inhibition of KCNQ alters potassium homeostasis, resulting eventually in OHC degeneration. Accordingyly, treatment of the auris interna with KCNQ modulators, in some cases activators, is contemplated within the scope of the embodiments disclosed herein as useful in the maintenance of sensory hair cell function in both vestibular and cochlear structures.
- Modulators of P2X channel function are also contemplated within the scope of the embodiments, for use, for example, in auris interna disorders, such as cochlear inflammation and noise-induced hearing loss.
- P2X channels which are gated by adenosine triphosphate, are present in a broad distribution of tissues, and are thought to play a role in peripheral and central neuronal transmission, smooth muscle contraction and inflammation.
- Purine nucleotides are thought to play a role in cochlear disease, where ATP plays a cytotoxic role via both apoptosis and necrosis due to the activation of P2X receptors.
- one embodiment is the use of modulators of P2X in the treatment of cochlear and vestibular disorders, including hearing and balance disorders.
- Antagonists and agonists Io P2X channels include BzATP, TNP-ATP, oc ⁇ -meATP, A-317491, PPADS, NF279, meSuramin, Reactive Blue II, RO-I , Adamantane amides, RO-3 and 4,5-diarylimidazolines.
- immunomodulators and/or aural pressure modulators modulate central nervous system activity.
- Contemplated for use with the formulations disclosed herein are agents which ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which inhibit the release of the neurotransmitter acetylcholine in the CNS.
- Anticholinergic agents are substances which block acetylcholine in the central and the peripheral nervous system. They treat balance disorders by suppressing conduction in vestibular cerebellar pathways, thus increasing motion tolerance.
- the anticholinergic is glycopyrrolate, homatropme, scopolamine or atropine. In some embodiments, the anticholinergic is glycopyrrolate. In some embodiments, the anticholinergic is homatropine. In some embodiments, the anticholinergic is scopolamine. In some embodiments, the anticholinergic is atropine.
- agents which ameliorate otic disorders including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which block the action of neurotransmitters in the CNS. Histamine is a neurotransmitter in the CNS. Accordingly, some embodiments incorporate the use of agents which modulate histamine receptors (e.g. the Hi receptor, H 2 receptor, and/or the H* receptor). 1 « some embodiments, antihistamines are as described herein.
- Calcium Channel Blockers Contemplated for use with the formulations disclosed herein are agents wliieh ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which block or antagonize Ca+ channels * Calcium channels are channels formed in the plasma membrane of neurons (amongst other cells) by integral membrane proteins. These channels conduct Ca ⁇ through a cell's plasma membrane. In neurons, the flow of Ca 2+ is partly responsible for creating and propagating action potentials in neurons. It can also be responsible for the release of certain neurotransmitters.
- the calcium channel antagonist is cinnarizine, flunarizine, or nimodipine.
- the calcium channel antagonist is cinna ⁇ zine.
- the calcium channel antagonist is flunarizine.
- the calcium channel antagonist is nimodipine.
- Other calcium channel blockers include verapamil, diltiazem, omega-conotoxin, GVlA, amlodipine, felodipine, iacidipine, mibefradil, NPPB (5-Nitro-2-(3- phenylpropylamino)benzoic Acid), flunarizine, and/or combinations thereof
- Contemplated for use with the formulations disclosed herein are agents which ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which modulate the action of GABA receptors in the CNS.
- GABA or ⁇ -aminobutyric acid, is an inhibitory neurotransmitter in the CNS. It acts at inhibitory synapses of both pre- and postsynaptic neuronal processes.
- GABA GABA ⁇ receptor, the GABA B receptor, and the CfABAc receptor
- GABA ⁇ receptor the GABA ⁇ receptor
- GABA B receptor the GABA B receptor
- CfABAc receptor the receptor for GABA
- some embodiments incorporate the use of agents which increase or decrease the sensitivity of the GABA receptors, or activate the GABA receptors by mimicking GABA.
- the benzodiazepine class of therapeutic agents are agonists of the GABA A receptor.
- a benzodiazepine binds to the GABA A receptor it induces a conformational change which increases the affinity of GABA for its receptor.
- the result of the increase in the binding of GABA is an increase in the frequency with which the Cl- channels in the neurons open. This causes
- the benzodiazepine is selected from the group consisting of: alprazolam, bromazepam, brotizolar ⁇ , chlordiazepoxide, clonazepam, clorazepate, diazepam, estazolam, fiunitrazepam, flurazepam. loprazolam, lorazepam,
- the GABA receptor modulator is a loop diuretic.
- the loop diuretic is furosemide, bumetanide, or ethacrynic acid.
- the loop diuretic is turosemide. In some embodiments, the loop diuretic is bumetanide. In some embodiments, the loop diuretic is ethacrynic acid. Furosemide, for example, binds to the GABA A receptor and reversibly antagonizes G ⁇ B ⁇ -evoked currents of the ⁇ 6, ⁇ 2, aud v2 receptors.
- useful loop diuretics include, but are not limited to, furosemide, bumetanide, and ethacrynic acid.
- the modulator of a GABA receptor is a GABA analogue.
- GABA analogues mimic G ⁇ BA.
- the receptor acts as though GABA is binding to it and the receptor is activated.
- the GABA analog is gabapentin, pregabalin, muscimol, or baclofen.
- the GABA analog Ls gabapentin.
- the G ⁇ B ⁇ analog is pregabalin. 1 « some embodiments, the GABA analog is muscimol.
- the GABA analogue is baclofen. Baclofen is an analogue of GABA which binds to and activates the GABA 8 receptor. Muscimol is also an analogue of GABA. It agonizes the GABA ⁇ receptor.
- Contemplated for use with the formulations disclosed herein are agents which ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CMS) activity. Accordingly, some embodiments incorporate the use of agents which inhibit the reuptake of neurotransmitters in the CNS. In some embodiments, the
- neurotransmitter reuptake modulator is an antagonist of a neurotransmitter reuptake target, partial agonist, inverse agonist, neutral or competitive antagonist, allosteric antagonist, and/or orthosteric antagonist.
- Neurotransmitter reuptake inhibitors inhibit the reuptake of neurotransmitters into presynaptic cells of the CNS. This increases the concentration of neurotransmitter available to stimulate post-synaptic cells of the CTNS.
- the neurotransmitter reuptake inhibitors are tricyclic antidepressants.
- Tricyclic antidepressants work by inhibiting the re-uptake of the neurotransmitters norepinephrine and serotonin by pre-synaptic cells. This increases the level of serotonin and/or norepinephrine available to bind to the postsynaptic receptor.
- the tricyclic antidepressant is amitriptylme, nortriptyline, or trimipramine.
- the tricyclic antidepressant is amitriptyline.
- the tricyclic antidepressant is nortriptyline.
- the tricyclic antidepressant is trimipramine.
- the neurotransmitter reuptake inhibitor is a selective serotonin reuptake inhibitor.
- SSRIs By inhibiting the reuptake of serotonin into the presynaptic cells, SSRIs increase the extracellular level of serotonin. This increases the level of serotonin available to bind to the postsynaptic receptor. SSRIs are hypothesized to stimulate new neural growth within the inner ear.
- the selective serotonin reuptake inhibitor is fluoxetine, paroxetine, or sertraline. 1 « some embodiments, the selective serotonin reuptake inhibitor is fluoxetine. In some embodiments, the selective serotonin reuptake inhibitor is paroxetine. In some embodiments, the selective serotonin reuptake inhibitor is sertraline.
- a ligand e.g. a tachykinin peptide, substance P, neurokinin A, and neurokinin B
- a neurokinin receptor e.g. a tachykinin peptide, substance P, neurokinin A, and neurokinin B
- a neurokinin receptor e.g. a tachykinin peptide, substance P, neurokinin A, and neurokinin B
- a ligand e.g. a tachykinin peptide, substance P, neurokinin A, and neurokinin B
- the activation of phospholipase C produces inositol triphosphate.
- the neurokinin receptor is the NK] receptor, the NK2 receptor, the NK3 receptor, or combinations thereof, In some embodiments, the neurokinin receptor is the NKl receptor. In some embodiments, the antagonist of the NKl receptor is vestipitant.
- the SSRJ inhibitor is administered in combination with a neurokinin receptor antagonist.
- the SSRl is paroxetine and the neurokinin receptor is NKl .
- the NKl receptor antagonist is vestipitant.
- the co-administration of paroxetine and vestipitant treats, and/or the symptoms of tinnitus.
- ⁇ 00423 ⁇ Contemplated for use with the formulations disclosed herein are agents which ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which decrease the rate of the depolarization and repolarization of neurons by, for example, blocking the Na ' channels in cell membranes.
- CNS central nervous system
- the CNS modulator is a local anesthetic.
- the local anesthetic is selected from the group consisting of: betxzoeain ⁇ , earu ' caine, cinchocaine, cyclomethycame, lidocaine, prilocaine, propxycaine, proparacaine, tetracaine, tocainide. and trimecaine.
- the local anesthetic is lidocaine.
- the local anesthetic is tocainide.
- Contemplated for use with the formulations disclosed herein are agents which ameliorate otic disorders, including vestibular disorders and/or tinnitus, through local modulation of central nervous system (CNS) activity. Accordingly, some embodiments incorporate the use of agents which block or antagonize Na+ channels.
- Sodium channels are channels formed in the plasma membrane of neurons (amongst other cells) by integral membrane proteins. These channels conduct Na + through a cell's plasma membrane, in neurons, the flow of Na ' is partly responsible for creating and propagating action potentials in the neurons.
- the sodium channel blocker is carbamazepine, oxearbazepine, phenytein, valproic acid, or sodium valproate. In some embodiments, the sodium channel blocker is carbam&zepine. Tn some embodiments, the sodium channel blocker is oxcarbazepine. In some embodiments, the sodium channel blocker is phenytein, in some embodiments, the sodium channel blocker is valproic acid. In some embodiments, the sodium channel blocker is sodium valproate.
- the Na- channel blocker is vinpocetine ((3a, 16a)-Eburnamenine-l 4- carboxylic acid ethyl ester); sipatrigine (2 ⁇ (4-Methylpiperazin-1-yl)-5-(2,3,5-trichlorophenyl)- pyrimidin-4-amine); amiloride (S.S-diamino-N ⁇ aminoiminomethyO- ⁇ -chloropyrazinecarbox amide hydrochloride); carbamazepine (5H-dibenzo[b,f]azepine-5-carboxamide); TTX (octahydro-12- (hydroxymethyl)-2-imino-5,9: 7, 1 Oa-dimethan.
- RS100642 (l-(2,6-dimethyl-phenoxy)-2-ethylaminopropane hydrochloride); mexiletine ⁇ (l-(2,6-dimethylphenoxy)-2-aminopropane hydrochloride)); QX -314 (N-(2,6- Dimethylphenylcarbamoylmethyl)triethylammonmm bromide); pheaytoin (5,5- diphenylimidazoHdiHe-2,4-dione); lamotrigine (6-(2,3-dichloropbenyl)-l ,2,44riazine-3,5-diamine); 4030W92 (2,4-diamino-5-(23-dichioiOphenyl)-6-fl ⁇ or
- agents which decrease the rate of the depolarization are provided.
- the local anesthetic is selected from the group consisting of: benzocaine, earticaine, cinchocaine, cyclomethycaine, lidocaine, prilocaine, propxycaine, proparacaine, tetracaine, tocainide, and trimecaine.
- the local anesthetic is lidocaine.
- the local anesthetic is tocainide.
- the antimicrobial agent is an antibacterial agent, an antifungal agent, an antiviral agent, an antiprotozoal agent, and/or an antiparasitic agent.
- Antimicrobial agents include agents that act to inhibit or eradicate microbes, including bacteria, fungi, viruses, protozoa, and/or parasites. Specific antimicrobial agents are used to combat specific microbes. Accordingly, a skilled practitioner would know which antimicrobial agent would be relevant or useful depending on the microbe identified, or the symptoms displayed,
- the antimicrobial agent is a protein, a peptide, an antibody, DNA, a carbohydrate, an inorganic molecule, or an organic molecule.
- the antimicrobial agents are antimicrobial small molecules.
- antimicrobial small molecules are of relatively low molecular weight, e.g., less than 1,000, or less than 600-700, or between 300-700 molecular weight.
- Antibacterial agents include amikacin, gentamicin, kanamycin, neomycin, netilmicin, streptomycin, tobramycin, paromomycin, gcldanmycin, herbimycin, loracarbef, ertapenem, doripenera, imipenem, cilastatin, meropenem, cefadroxil, cefazolin, cefalofin, cefalexin, cefaclor, cefamandole, cefoxitin, defprozil, cefuroxime, cefixime, cefdinir, cefditoren, cefoperazo ⁇ e, cefotaxime, cefpodoxime, ceftazidime, cefHbuten, ceftizoxime, ceftriaxone,titiepime, ceftobiprole.
- teicoplanin vancomycin, azithromycin, clarithromycin, dirithromycin, erythromycin, roxkliromycin, troleandomycin, telithromycin, spectinomycin, aztreonam, amoxicillin, ampicillin, azlocillin, carbenicillin, cloxacillin, dicloxacillin, flucloxacillin, mezlocillin, meticillia nafcillin, oxacillin, penicillin, piperacillin, ticareillan, bacitracin, colistin, polymyxin B, ciprofloxacin, enoxacin, gatifloxacin, levofloxacin, lomefloxacin, moxifloxacin.
- norfloxacin ofloxacin, trovfloxacin, mafenide, prontosil, sulfacetamide, sulfametliizole, sulfanimilimde, sulfasalazine, s ⁇ lfsioxazole, trimethoprim, demeclocycline, doxycyciine, minocycline, oxtetracycline, tetracycline,
- Antiviral agents include acyclovir, famciclovir and valacyciovir.
- Other antiviral agents include abacavir, acyclovir, adfovir, amantadine, amprenavir, arbidol., atazanavir, artipla, brivudine, cidofovir, combi ⁇ dr, edoxudine, efavirenz, cmtiicitabine, enfuvirtide, entecavir, fomvirsen, fosarnprenavir, foscarnet, fosfonet, ganciclovir, garda&il, ibacitabine, imunovir, idoxuridine, imiquimod, indinavir, inosine, integrase inliibitors, interferons, including interferon type 111, interferon type TT, interferon type I, lamiv ⁇ dine, lopin
- Antifungal agents include amrolfine, utenaline. naftifine, terbinafine, flucytosine, fluconazole, itraconazole, ketoconazole. posaconazole, ravuconazole, voriconazole, clotrimazole, econazole, miconazole, oxiconazole, sulconazole, terconazole, tioconazole, nikkomycin Z, caspofungin, raicafungin, anidulafungin, amphotericin B, liposomal nystastin, pimaricin, griseofulvin, ciclopirox olamine, haloprogin, tolnaftate, undecylenate, clioquinol, and combinations thereof.
- Antiparasitic agents include amitraz, amoscanate, avermectin, carbadox, diethylcarbamizine, dimetridazole, diminazene, ivermectin, macrofilaricide, malathion, mitaban, oxamniq ⁇ ine, pe ⁇ ttethrin, praziquantel, prantel pamoate, selamectin, sodium stibogluconate, thiabendazole, and combinations thereof.
- pharmaceutically active metabolites, salts, polymorphs, prodrugs, analogues, and derivatives of the antimicrobial agents discussed above that retain the ability of the parent antimicrobial agents to treat otic disorders of the ear are also useful in the formulations disclosed herein.
- immunomodulators and/or aural pressure modulators relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria.
- agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of agents which prevent and/or ameliorate the damage caused by free radicals. In some embodiments, the agents which prevent artd/or ameliorate the damage caused by free radicals is an antioxidant.
- Antioxidants are also useM as protectants against ototoxic agents through the prevention of reactive oxygen species, neutralization of toxic products or blockage of the apoptosis pathway.
- Resveratroi (3,5,4 1 -Trihydroxystilber ⁇ e), a representative example of an antioxidant, exerts its effects through a variety of pathways, including the inhiition of MnSOD, which reduces superoxide to H 2 O 2 , which inhibits free radical chain reactions, reducing superoxide levels in the celi.
- resveratroi has been implicated in preventing neuronal cell dysfunction and cell death.
- antioxidants include but are not limited to vitamin E (tocopherol), vitamin C (ascorbic acid), glutathione, lipoic acid, alpha lipoic acid, uric acid, carotenes, ubiquinoL melatonin, locolrienols, selenium, fiavonoids, polyphenols, lycopene, lutein, ligiian, butyl hydroxytoluene, coenzyme QlO, salicylate, or combinations thereof.
- vitamin E tocopherol
- vitamin C ascorbic acid
- glutathione glutathione
- lipoic acid alpha lipoic acid
- uric acid carotenes
- ubiquinoL melatonin carotenes
- locolrienols selenium
- fiavonoids polyphenols
- lycopene lutein
- ligiian butyl hydroxytoluene
- coenzyme QlO salicylate
- nitrones act synergisticaliy with antioxidants. In certain embodiments, nitrones trap free radicals. In some embodiments, a nitrone (e.g. alpha-phenyi-tert- b ⁇ tylnitrone (PBN), allpurinol) is co-adruinistered with an antioxidant. In certain embodiments, a nitrone co-administered with an antioxidant treats acute acoustic noise-induced hearing loss.
- PBN alpha-phenyi-tert- b ⁇ tylnitrone
- the antioxidant is N-acetylcysteine; vitamin E (tocopherols and tocotrienols); vitamin C; vitamin A; lutein,' selenium glutathione; melatonin; a polyphenol; a carotenoid (e.g. lycopene, carotenes); coenzyme Q-10; Ebselen (2-phenyl ⁇ l « 2-benzisoseienazol- 3(2H)-one (also called PZ 51 or DR3305); L-methionine; azulenyl nitrones (e.g.
- Contemplated for use with the formulations disclosed herein are agents that modulate the production of free-radicals and/or inhibit damage to the mitochondria. Accordingly, some embodiments incorporate the use of agents which modulate glutamate receptors.
- the glutamate receptor is the AMPA receptor, the NMDA receptor, and/or a group ⁇ I or III mGlu receptor.
- a glutamate reptor modulator is as described herein.
- agents which prevent and/or ameliorate the damage caused by free radicals is an iron chelator.
- the iron chelator, deferoxamine, prevents ototoxic damage to the ear resulting from treatment with neomycin when it is co-administcred with neomycin.
- the iron chelator is desferoxamine (DFO); hydroxybenzyl ethylene diamine; fullerenol-1, pyrrolidine dilhioearbamate; desferal; Vk-28 (5-j4-(2-hydroxyethyl) piperazine-1-ylmethyl]-quinolme-8-ol); clioq ⁇ inol; echioochrome; PIH (pyridoxal isomcotinoyl hydrazone); deferasirox; HBED (N,N'-bis (2-hydroxybenzyi) ethylenediamine-N,N'-diacetic acid); Sill (salicylaldehyde isonicotinoyl hydrazone): deJferiprone; Ll (1,2-dimethyl-3-hydroxy- 4- pyridone); Kojic acid (5-hydroxy-2-hydroxymethyl-4-pyrone); deferoxamine; 2,3- dihydr ⁇ xybenz
- agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents tliat modulate the activity of the mitochondria. In some embodiments, the agent which modulates the activity of the mitochondria is aceiylcamitine; lipoic acid; or combinations thereof.
- Nitric oxide is a neurotransmitter. It is synthesized by multiple nitric oxide synthases (NOS) from argmine and oxygen. It is also derived from the reduction of inorganic nitrate. In certain instances, it induces vasodilation; thus, increasing blood flow. In certain instances, it increases cochlear blood flow. In certain instances, NO damages blood vessel walls. In certain instances, NO ameliorates vascular protein leakage in the cochlea, In certain instances, NO increases the sensitivity of hair ceils. In certain instances, NO reacts with super-oxide to form the free radical peroxynitrite. Accordingly, some embodiments incorporate the use of agents that modulate nitric oxide and/or nitric oxide synthase (NOS).
- NOS nitric oxide synthase
- the agent that modulates NO and/or NOS is an antagonist of NO or NOS.
- the antagonist of NO a ⁇ d/or NOS is aminoguanidine; 1 -Amino-2- hydroxyguanidinep-toluensulfate; GED (guanidinoethyldisulfide); bromocriptine mesylate;
- d ⁇ xamethasone symmetric N ⁇ N ⁇ -Dimethyl-L-arginine
- ADMA asymmetric N G ,N ⁇ - Dimethyl-L-arginine
- L-NMMA N ⁇ -monomethyl-L-arginine
- L-N]VfEA N G -monoethyl-L- arginine
- D-MMA N G -monomethyl-D-arginine
- diphenyieneiodonium chloride 2-ethyl-2-tbiopseudourea; haloperidol; L-NIO (L-N 5 -(l- m ⁇ noethyl)ornithine); MEG (methylecgonidine); SMT (S-methylisothiourea sulfate); SMTC (S- methyl-L-t ⁇ iiocitrullme); 7-Ni (7-nitroindaz ⁇ le); nNOS inhibitor I ((4S)-N-(4-Amino- 5[aminoetbyl]amtnopentyl)-N'-niuOguanidme); 1,3-PBITU (S,S'-l ,3-Phenylene-bis(1,2- ethanediyl)-bis-isothiourea): L-thiocitrulline; TRJM (l-(2-trifluorometnylphenyl)
- the agent that modulates NO and/or NOS is an agonist of NO and/or NOS, or a donor of NO.
- the agonist of NO and/or NOS, or donor of NO is S-NC (S-nitrosocysteine); NTG (nitroglycerine); SNP (sodium nitroprusside); thapsigargirs; vascular endothelial growth factor (VEGF); bradykinin; ⁇ TP; sphingosine-1 -phosphate; estrogen;
- Hie sirruias (or Sir2 proteins) comprise class III of the histone deacetylases (HUACs). While they are classified as protein deacetylases some also function as mono-ADP- ribosyltranslerases. Each sirtuin protem has a homologous core sequence of 250 amino acids. This sequence is highly conserved over multiple species. Further, in order to catalyze the deacetylation of a protein, each sirtuin requires NAD' as a cofactor. There are seven members of the family: Sirtl . Sirt2, Sin3, Sirt4, Sirt5, Sirt6, and Sirt7. Sirtl and Sirt3 are protein deacetylases. Sirt2 is involved in mitosis.
- HUACs histone deacetylases
- Agonism of Sirtl yields multiple benefits which have previously been identified in subjects undergoing caloric restriction. These benefits include, but are not limited to. decreased glucose levels and improved insulin sensitivity, increased mitochondrial activity, and decreased adiposity (due to the Sirtl mediated repression of PPAR- ⁇ ). Decreases in glucose levels and adiposity can contribute to the amelioration of presbycusis as diabetes and atherosclerosis are both factors which contribute to the development and progression of presbycusis. [00451] Sirtl can prevent apoptosis by deacetylating the pro-apoptotic genes p53 and Ku-70.
- Additional substrates for Sirtl include, but are not limited to, the transcription factors NFKB, FoxOl, Fox03a, Fox04, Fox05; the transcription repressor Hie 1; and Pgc-l ⁇ . which regulates, among other cellular functions, adaptive thermogenesis, glucose metabolism, and triglyceride metabolism, Agonism of Sirt3 results in increased cellular respiration and a decrease in the production of reactive oxygen species (ROS).
- ROS reactive oxygen species
- NAD nicotinamide adenine dimicleotidc
- the sirtuin hydrolyzes NAlT by breaking the glycosidic bond between nicotinamide and ADP-ribose.
- the acetyl group of the acetylated protein is then, transferred to ADP-ribose.
- the deacetylated protein, and 2'-O-acetyl-ADP-ribose are released.
- resveratrol (/7Y ⁇ Mv ⁇ r-3,5,4 ⁇ -trihydroxystilbene) decreases apoptosis. Il also increases glulamate uptake and thus ameliorates excitotoxicity. Further, administration of resveratrol results in lower levels of reactive oxygen species (ROS) and thus ameliorates damage caused by ischemia, excitotoxicity. ototoxicity caused by cisplatin and aminoglycosides, acoustic trauma and presbycusis.
- ROS reactive oxygen species
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deacetylation reactions.
- the agent which modulates siituin catalyzed deacetylation reactions is a stilbene.
- the stilbene is frvmv-stilbene, m-stilbene. resveratrol, ptceataanol, rhapontin, deoxyrhapontin, butein, or combinations thereof.
- the stilbene is resveratroi .
- the stilbene is an analog of resveratroi.
- the analog of resveratrol is SRT-501 (RM-i 821 ).
- RM-i 821 For additional analogs of resveratrol see U.S. Patent App. Pub. No. 2006/0276393, which is hereby incorporated by reference for this disclosure.
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuki catalyzed deacetylation reactions.
- the agent which modulates sirtuin catalyzed deacetylation reactions is a chalcone.
- the chalcone is chalcon; isoliquirtigen; butein; 4,2',4'-trihydroxychalcone; 3,4,2',4',6 S - pentahydroxychalcone; or combinations thereof.
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents tfos modulate sirtuin catalyzed deacetylation reactions. In some embodiments, the agent which, modulates sirtuin catalyzed deacetylation reactions is a flavone.
- the flavone is flavone, morin, f ⁇ setin; luteolin; quercetin; kaempferol: apigenin; gossypetin; myricetin; 6-hydroxyapigenin; 5-hydroxyflavone; 5,7,3 ⁇ 4 ⁇ 5' ⁇ pentahydroxyfJavone; 3.7,3 ⁇ 4',5 * - pentahydroxyflavone; 3,6,3 ⁇ 4'-teJ ⁇ ahydroxyilavone; 7,3 ⁇ 4 ⁇ 5Metrdhydr ⁇ xyflavone; 3,6,2 ⁇ 4'- tetrahydroxyflawne; 7,4'-dihydroxyflavone: 7.8,3' ( 4'-tetrahydroxyflavone; 3,6,2 ⁇ 3'- tetrahydroxyflavone; 4 ' -hydroxyfiavone; 5-hydroxyflavone; 5,4'-dihydroxyflavone; 5,7- dihydroxyflavone; or combination thereof.
- f00459J Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deacetylation reactions.
- the agent which modulates sirtuin catalyzed deacetylation reactions is an i.soflavone.
- the isoflavone is daidzein, genistein, or combinations thereof.
- [0046Oj Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deacetylation reactions.
- the agent which modulates sirtuin catalyzed deacetylation reactions is a flavanone.
- die flavanone is naringenin; flavanone; 3,5,7,3 ⁇ 4'-pentahydroxyflavanone; or combinations thereof.
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deaceiylation reactions. In some embodiments, the agent which modulates sirtuin catalyzed deacetylation reactions is an anthocyanidin. In some
- the anthocyanidin is pelargonidin chloride, cyanidin chloride, delphiuidin chloride, or combinations (hereof.
- Contemplated for use with die formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and-'or hair cells of the au ⁇ s due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deacetylation reactions. In some embodiments, the agent which modulates sirtuin catalyzed deacetylation reactions is a calechin.
- the eaiechin is (-)-epicatechin (Hydroxy Sites: 3,5,7,3',4'); (-)-catechin (Hydroxy Sites: 3,5,7,3'.4'); (-)-galiocateehin (Hydroxy Sites: 3,5,7,3 ⁇ 4',5') (+)-catechin ⁇ I lydroxy Sites: 3,5,7,3',4'); (+)- epicatechin (Hydroxy Sites: 3,5,7,3',4'); or combinations thereof.
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and-'or hair cells of the a ⁇ ris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents that modulate the catalytic rate of sirtuin catalyzed deaeetylation reactions.
- the agent which modulates the catalytic rate of sirtuin catalyzed deacetylation reactions is dipyridamole, ZM 336372 (3-(dimetljylamino)-N-[3-
- Contemplated for use with the formulations disclosed herein are agents that relieve, prevent, reverse or ameliorate the degeneration of neurons and/or hair cells of the auris due to free radicals or the dysfunction of the mitochondria. Accordingly, some embodiments incorporate the use of one or more agents the modulate sirtuin catalyzed deacetylation reactions.
- the agent that modulates sirtuin catalyzed deacetylation reactions is a nicotinamide binding antagonist.
- the nicotinamide binding antagonist is isonicolinamide or an analog of isonicotinamide.
- the analog of isonicotinamide is ⁇ -1 '-5-raethyl- nicotinamide-2'-deoxyribose; ⁇ -D-1 '-5-methyl-nico-tinamide-2'-deoxyribofuranoside; ⁇ -l'-4,5- dimethyl ⁇ nicotinamide-2'-de ⁇ oxyribose; or ⁇ -D-1 '-4,5-dimethyl-nicotinamide-2'- deoxyribofuranoside.
- Lsonicotinamide see U.S. Pat. Nos. 5,985,848;
- agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs and neurons in the inner ear are agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs and neurons in the inner ear. Accordingly, some embodiments incorporate the use of agents that modulate potassium ion concentrations. In some embodiments, the agents that modulate potassium ion concentrations are agonists or antagonists of potassium ion channels.
- Potassium ion channels are channels that regulate the flow of potassium ions into and out of ceils. In the cochlea the transduction current through the sensory cells is carried by potassium ions and depends on. the high concentration of potassium ions in the end ⁇ lymph. Mutations in the genes encoding potassium channel protein result in both acquired and congenital hearing loss.
- KCNQ fa ⁇ u ' ly of potassium channels is a family of delayed rectifier voltage-gated potassium channels found in the cochlea.
- KCNQl subunits form potassium channels in vestibular dark cells and marginal cells of the stria vascularis. These channels regulate the level of potassium in endolymph.
- KCNQ4 subunits form channels hair cells. Mice with genes encoding KCNQ subunits knocked-out display a hearing loss during development, starting at four weeks of postnatal life.
- the agent that modulates a potassium channel is an agoinst of a potassium channel (e.g. a potassium channel opener).
- the agonist of a potassium channel is nicorandil; minoxidil, ievcromakaUm; lemakalim; cromakalim; L-735,334 (14- hydroxy C ⁇ F-603 oleate); retigabine; flupirline; BMS-204352 (3S)-( ⁇ )-(5-Chloro-2- methoxypheny])-l ,3-diliydro-3-fluoro-6-(trifluoromethyl)-2H-indole-2-one); DMP-543 (10,10- bis((2-fluoro-4-pyridinyl)methyl)-9(10H)-antliracenone); or combinations thereof.
- the agent that modulates a potassium channel is an antagonist of a potassium cliannel (e.g. a potassium channel blocker).
- the antagonist of a potassium clxan ⁇ el is linopirdine; XE991 (10,10-bis(4-pyridJnyimeth>'I)-9(l()H)-antliracenone); 4- AP (4-aminopyridine); 3,4-DAP (3,4-Diaminopyridinc); E-4031 (4'-[[l-[2-(6-methyl-2- pyridyl)ethyl]-4-piperidinyl]carbonyl]-.methanesulfonanilide); DIDS (4,4'-diisothiocya ⁇ .ostilbene- 2 > 2'-disulfonic acid); Way 123,398 (N-meihyl-N-(2-(methyl(l-methyl-l H-
- J00469 ⁇ Contemplated for use with the formulations disclosed herein are agents for modulating ion channels. Accordingly, some embodiments incorporate the use of agents that modulate the concentration of ions. In some embodiments, the agents that modulate the concentration of ions are agonists or antagonits of purigenic receptors.
- Purigenic receptors are a family of plasma membrane-bound receptors.
- the family includes the P2X, P2Y, and Pl receptors.
- the P2X receptors comprise ion channels. When AlT binds to the receptor the channel opens.
- the P2Y receptors comprise G-coupled protein receptors.
- the ligands for these receptors are ATP, ADP, UTP, UDP, UDP-glucose.
- the Pl receptors comprise G-coupled protein receptors.
- the ligand for these receptors is adenosine. Purigenie receptors regulate ion homeostasis in the car.
- the agonist of a purigenic receptor is ATP; AI)P; UTP; UDP; UDP- glucose; adenosine; 2-MeSAIP; 2-MeSAOP; o ⁇ meATP; dATPoS; ATPyS; Bz-AIP; MRS2703 (2- MeSADP with the beta-phosphate group blocked by a l-(3,4-dimethyloxyphenyl)eth-l -yi phosphoester)): dcnufosol tetrasodiuin; MRS2365 ([[(lR,2R,3S,4R,5S)-4-[6-amino-2-(metliylthio)- 9H-purin-9 -yIJ-2,3-dihydroxybic
- the antagonist of a purigenic receptor is A-317491 ((5-([(3- Phenoxybenzyl)[(l S)-1 ,2,3,4-tetrahydro-l -naphthalenyl]amino]carbonyl)-l ,2.4- benzenetricarboxylic acid)); RO-3 (Roche); suramin; PPADS (pyridoxalphosphate-6-azophenyl- 2',4'-disulfonic acid); PPNDS (P> ⁇ idoxal-5 l -phosphate-6-(2 l -naphthylazo-6 l -nitro-4 l ,8 1 -disulfonate) tetrasodium salt); DIDS; pyridoxal-5 -phosphate; 5-(3-bromqphenyl)-1,3-dihydro-2i/-benzofiiro- [3,2-e]-1,4-diaze
- RNA interference is optionally utilized.
- the agent that inhibits or down-regulates the target is an siRNA molecule.
- the siRN ⁇ molecule is as described herein.
- any otic active agent ⁇ e.g., an im ⁇ nmoniodulator or an auris pressure modulator
- an otic agent is administered with an anti-emetic agent (e.g., when a balance disorder is accompanied by nausea).
- an otic agent is administered in combination with one or more otoprotectant (e.g., when the administration of a cytotoxic agent is accompanied by ototoxicity).
- an otic agent is administered in combination with, for example, an anti-emetic, an antimicrobial agent, a nitric oxide synthase inhibitor, an antioxidant, a neurotransmitter reuptake inhibitor, an otoprotectant, a homeostasis modulator (e.g., ion/ fluid (e.g., water) homeostasis modulator) or the like.
- an anti-emetic e.g., an antimicrobial agent, a nitric oxide synthase inhibitor, an antioxidant, a neurotransmitter reuptake inhibitor, an otoprotectant, a homeostasis modulator (e.g., ion/ fluid (e.g., water) homeostasis modulator) or the like.
- a homeostasis modulator e.g., ion/ fluid (e.g., water) homeostasis modulator
- Anti-Emetic agents are optionally used in combination with any otic formulations disclosed herein.
- Anti-emetic agents include antihistamines and central nervous agents, including antipsychotic agents, barbiturates, benzodiazepines and phenothiazines.
- Other anti-emetic agents include the serotonin receptor antagonists, which include dolasetron, grantsetron, ondansetron, (ropisetron, palonosetron, and combinations thereof; dopamine antagonists, including domperidone, properidol.
- haloperidol haloperidol, ehlorpromazine, promethazine, prochlorperazine and combinations thereof; cannabinoids, including dronabinol, nabilone, sativex, and combinations thereof; anticholinergics, including scopolamine; and steroids, including dexamethasone; trimethobenzarnine, emetrol, propofol, muscimol, and combinations thereof.
- Central Nervous System agents and barbiturates are useful in the treatment of nausea and vomiting symptoms that accompany an autoimmune otic disorder.
- an appropriate barbiturate and/or central nervous system agent is selected to relieve or ameliorate specific symptoms without possible side effects, including ototoxicity.
- targeting of the drugs to the round window membrane of the auris interna reduces possible side effects and toxicity caused by systemic administration of these drugs.
- Barbiturates which act as a central nervous system depressant, include allobarbitai, alphenal.
- amobarbital amobarbital, aprobarbital, baraexacione, barbital, bra ⁇ obarbital, butabarbital, butalbital, butallylonal, butobarbiUu, corvalol, crotylbarbital, cyclobarbital, cyclopal, ethallobarbital, febarbamate, heptabarbital, hexethal.
- hexobarbital metharbital, methohexital, methylphenobarbital, narcobarbitai, nealbarbital, pentobarbital, phenobarbital, primidone, probarbitaL propallylonal, proxibarbital, reposal, secobarbital, sigrnodal, sodium thiopental, talbutai, thialbarbital, thiaraylai, thiobarbital, thiobutabarbital, tuinaL valofane, vinbarbital, vinyibilal, and combinations thereof.
- benzodiazepines or phenothiazines.
- Useful benzodiazepines include, but are not limited to diazepam, lorazeparn, oxazepam, prazepam, alprazolam, bromazepam, chlordiazcpoxide, clonazepam, clorazepate, brotizolam, estazolam, flunitrazepara, flurazepam, loprazolar ⁇ , lormetazepam, midazolam, nimetazepam, nitrazepam, temazepam, triazolam, and combinations thereof.
- phenothiazines examples include prochlorperazine, chbrpromazine, promazine, triflupromazine, levopromazine, methotrimepramazine, mesoridazine, thiroridazitie, fluphenazine, perphenazine, flupentixol, trifluoperazine, and combinations thereof.
- Antihistamines act to inhibit the release or action of histamine.
- Antihistamines that target the Hl receptor are useful in the alleviation or reduction of nausea and vomiting symptoms that are associated with ALBD, other autoimmune disorders, as well as antiinflammatory disorders. Accordingly, some embodiments incorporate the use of agents which modulate histamine receptors (e.g. the Hi receptor, H ? receptor, and/or the H ? receptor).
- antihistamines include, but are not limited to, meclizine, diphenhydramine, loratadine and quetiapine.
- Other antihistamines include mepyramine, piperoxan, antazoline, carbinoxamine, doxylamine, clemastine, dimenhydrinale, pheniramine, chlorphenamine, chlorphenirar ⁇ ine, dexchlorpheniramine, brompheniramine, triprolidine, cyclizine, chlorcyclizine, hydroxyzine, promethazine, alimeraazine, trimeprazine, cyproheptadine, azatadine, ketotifen, oxatomide and combinations thereof.
- the 11 3 receptor antagonist is meclizine hydrochloride.
- the Hj receptor antagonist is promethazine hydrochloride.
- the H] receptor antagonist is dimenhydrinate.
- the H t receptor antagonist is diphenhydramine.
- the H 1 receptor antagonist is cinnarizine.
- the Hi receptor antagonist is hydroxyzine pamoate.
- IJ Antihistamines which target the H 1 receptor include, but are not limited to betahistine dihy ⁇ rochloride.
- Antimicrobial agents are also contemplated as useful with the formulations disclosed herein. In some embodiments, the antimicrobial agent is as described herein.
- otic formulations described herein e.g, aural pressure modulating formulations, immunomodulator formulations described herein
- corticosteroid agents which reduce or ameliorate symptoms or effects as a result of an autoimmune disease and/or inflammatory disorder, including AIED.
- Such autoimmune response are a contributing factor to otic disorders such as Meniere ' s disease.
- corticosteroids modulate the degeneration of neurons and/or hair ceils of the amis, and agents for treating or ameliorating hearing loss or reduction resulting from destroyed, stunted, malfunctioning, damaged, fragile or missing hairs m the inner ear.
- some embodiments incorporate the use of agents which protect otic hair cells from ototoxins.
- the agent which protects otic hair cells from ototoxins is a corticosteroid.
- Such steroids include prednisolone, dexamethasone, dexamethasone phosphate, beclomethasone, 21-acetoxypregnenolone,
- alclometasone algestone, amcinonide, beclomeihasone, betamethasone, budesonide,
- fluocinonide fluocortin butyl, fluocortolone, fluoiOinetholone, fluperolone acetate, fluprednidene acetate, fluprcdnisolonc, tlurandrcnohde, fluticasone propionate, formooortal, halcin ⁇ t ⁇ de, halobetasol propionate, halometasone, halopredone acetate, hydrocortamate, hydrocortisone, loleprednol etabonate, rnazipredone, medrysone. meprednisone, methylprednisolone, mometasone furoate.
- paramethasone prednicarbate, prednisolone, prednisolone 25-diethylaniino-acetate, prednisolone sodium phosphate, prednisone, prednival, prednylidene, rirnexolone, tixocoriol, triamcinolone, triamcinolone acetonide, triamcinolone benetonide, triamcinolone hexacetonide and combinations thereof.
- triaraiemolone actenoide and dexamethasone protect oiic hair cells from damage caused by the naturally occurring toxin 4-hydroxy-2,3-tx>nenal (HNfE), which is produced in the inner ear in response to oxidative stress.
- any otic formulation described herein e.g. auris sensory cell modulating agent formulations disclosed herein
- otoprotectants that reduce, inhibit or ameliorate the ototoxicity of agents such as chemotherapeutic agents and/or antibiotics as described herein, or reduce, inhibit or ameliorate the effects of other environmental factors, including excessive noise and the like.
- otoprotectants include, and are not limited to, thiols and/or thiol derivatives and'or pharmaceutically acceptable salts, or derivatives (e.g. prodrugs) thereof (e.g., D-methionine, L-methionine, ethionine, hydroxy! methionine, methionirtol.
- amifostinc mesna (sodium 2-sultanylethanesuifonate), a mixture of D and L methionine, normethionine, homomethionine, S-adenosyl-L -methionine), dielhyldithiocarbamate, ebselen (2-phenyl-l, 2- benzisoselenazol-3(2H)-one), sodium thiosulfate, /MvI-11 1 (a cell permeable JNK inhibitor, (Laboratoires Auris SAS)), leucovorin, leucovorin calcium, dexrazoxane, piracetam, Oxiraeetam, AniraceUirn, Pramiracetam, Phenylpiracetam (Carphedon), Etiracetam, Levetiracetam, Nef ⁇ racetam, Nieoraeetam, Rolztracetara, Nebracetam, Fas
- Oloprotectants allow for the administration of ehemotherapeutic agents and/or antibiotics at doses that are higher than maximal toxic doses; the chemotherapeutic agents and/or antibiotics would otherwise be administered at lower doses due to ototoxicity.
- Oloprotectants when optionally administered by itself, also allow for the amelioration, reduction or elimination of the effect of e ⁇ v ⁇ ronmental factors that contribute to loss of hearing and attendant effects, including but not limited to noise-induced hearing loss and tinnitus.
- the amount of otoprotectant in any formulation described herein on a mole:raole basis in relation to the ototoxic chemotherapeutic agent (e.g. cis piatin) and/or an ototoxic antibiotic (e.g. gentamicin) is in the range of from about. 5: 1 to about 200: 1 , from about 5: 1 to about I (K): 1 , or from about 5:1 to about 20:1,
- gentamicin is about. 50:1, about 20:1 or about 10:1.
- Any the auris sensory cell modulating agent formulation described herein comprises from about 10 mg/mL to about 50 mg/mL, from about 20 mg/mL to about 30 mg/mL, or from about 25 mg/mL of otoprotectant.
- Chemotherapeuctie agents are also contemplated for use with the formulations disclosed herein.
- Chemolherapeutic agents act by killing cancer cells or microorganisms, and may include antineoplastic agents that target, cancer or malignant cells.
- Some chemotherapeutic agents, either alone or in combination, are also ototoxic.
- cisplatin is a known cocbJeotoxic agent.
- use of cisplatin in combination with antioxidants are protective and lessen the ototoxic effects of the chemotherapeutic agent.
- the localized application of the cytotoxic drug may lessen the ototoxic effects that might otherwise occur through systemic application through the use of lower amounts with maintained efficacy, or the use of targeted amounts for a shorter period of time. Accordingly, a skilled practitioner choosing a course of therapy for tumor growth will have the knowledge to avoid or combine an ototoxic compound, or to vary the amount or course of treatment to avoid or lessen ototoxic effects.
- Chemotherapeutic agents that are used in combination with the formulations disclosed herein include, for example, but are not limited to adriamycin, imidazole carboxamide,
- cyclophosphamide mechlorethamine, chlorambucil, melphalan, daunorubicin, doxorubicin, epirubicin, idarubicin, mitoxanthrone, vairubicin, paclitaxel, docetaxel, etoposide, teniposide, tafluposide, azacitidine, azathioprine, capecitabme, cytarabine, doxifluridine, fluorouracil, gemcitabine, mercaptopurine, methotrexate, tiog ⁇ anine, bleomycin, carboplalin, cisplatin, oxaliplatin, all-trans retinoic acid, vinblastine, vincristine, vindesine, vinorelbine, and combinations thereof.
- Homeostatis modulators are contemplated as useful with the formulations described herein.
- Homeostasis modulators include ion and fluid (e.g. water) homeostasis modulators.
- homeostasis modulators include Na/K-ATPase modulators, ENaC modulators, vasopressin receptor modulators, diuretics or the like as described herein.
- Na/K-ATPase modulators are contemplated for use with the formulations disclosed herein. Cochlear homeostasis is dependent on the electrolyte composition of the endolyniph, which is regulated by an active exchange of Na 1 and K + via a ATPase.
- Na/K-ATPase modulators include, and are not limited to, niraodipine (a sodium-potassium adenosine triphosphatase stimulator), ouabain, and furosemide.
- I00492J Also contemplated herein are the use of devices for the delivery of the pharmaceutical formulations disclosed herein, or alternatively for the measurement or surveillance of the function of the auris formulations disclosed herein.
- devices for the delivery of the pharmaceutical formulations disclosed herein, or alternatively for the measurement or surveillance of the function of the auris formulations disclosed herein.
- pumps, osmotic devices or other means of mechanically delivering pharmaceutical formulations are used for the delivery of the pharmaceutical formulations disclosed herein.
- Reservoir devices are optionally used with the pharmaceutical drug delivery units, and reside either internally along with the drug delivery unit, or externally of the auris structures.
- MRl magnetic resonance imaging
- 3 Tesla MRI devices 3 Tesla MRI devices
- the MRl devices for example, 3 Tesla MRI devices
- the pharmaceutical formulations disclosed herein See, Carfrae et ai. Laryngoscope 118:501-505 (March 2008).
- Whole body scanners, or alternatively cranial scanners, are contemplated, as well as higher resolution (7 Tesla, 8 Tesla, 9,5 Tesla or 11 Tesla for humans) are optionally used in MRl scanning.
- otic compositions that ameliorate or lessen otic disorders described herein.
- methods comprising the administration of said otic compositions.
- the compositions are sterilized. Included within the embodiments disclosed herein are means and processes for sterilization of a pharmaceutical composition disclosed herein for use in humans. The goal is to provide a safe pharmaceutical product, relatively free of infection causing micro-organisms.
- the U. S. Food and Drug Administration has provided regulatory guidance in the publication "Guidance for Industry: Sterile Drug Products Produced by Aseptic Processing" available at: http://w ⁇ vw.fda.gov/cder/guidance/5882M.htm, which is incorporated herein by reference in its entirety. No specific guidelines are available for safe pharmaceutical products for treatment of the inner ear.
- sterilization means a process used to destroy or remove microorganisms that are present in a product or packaging. Any suitable method available for sterilization of objects and compositions is used. Available methods for the inactivation of microorganisms include, but are not limited to, the application of extreme heat, lethal chemicals, or gamma radiation.
- a process for the preparation of an otic therapeutic formulation comprising subjecting the formulation to a sterilization method selected from heat sterilization, chemical sterilization, radiation sterilization or filtration sterilization. The method used depends largely upon the nature of the device or composition to be sterilized. Detailed descriptions of many methods of sterilization are given in Chapter 40 of Remington: The Science and Practice of Pharmacy published by Lippincott, Williams & Wilkins, and is incorporated by reference with respect to tills subject matter.
- This process takes place in an apparatus suitable for beating HEP A-filtered microorganism-free air to temperatures of at least 130-180 °C far the sterilization process and to temperatures of at least 230-250 °C for the depyrogenation process.
- Water to reconstitute concentrated or powdered formulations is also sterilized by autoclave.
- Chemical sterilization methods are an alternative for products that do not withstand the extremes of heat sterilization.
- a variety of gases and vapors with germicidal properties such as ethylene oxide, chlorine dioxide, formaldehyde or ozone are used as the anti- apoptotic agents.
- the germicidal activity of ethylene oxide arises from its ability to serve as a reactive alkylating agent.
- the sterilization process requires the ethylene oxide vapors to make direct contact with the product to be sterilized.
- One advantage of radiation sterilization is tJhe ability to sterilize many types of products without heat degradation or other damage.
- the radiation commonly employed is beta radiation or alternatively, gamma radiation from a 60 Co source.
- the penetrating ability of gamma radiation allows its use in the sterilization of many product types, including solutions, compositions and heterogeneous mixtures.
- the germicidal effects of irradiation arise from the interaction of gamma radiation with biological macromolecules. This interaction generates charged species and free radicals. Subsequent chemical reactions, such as rearrangements and cross-linking processes, result in the loss of normal function for these biological macromolecules.
- the formulations described herein are also optionally sterilized using beta irradiation.
- Filtration sterilization is a method used to remove but not destroy microorganisms from solutions.
- Membrane filters are used to filler heat-sensitive solutions. Such filters are thin, strong, homogenous polymers of mixed cellulosic esters (MCE), polyvirtylidene fluoride (PVF; also known as PVDF), or polyletrafluoroethylene (PTFE) and have pore sizes ranging from 0.1 to 0.22 ⁇ m. Solutions of various characteristics are optionally filtered using different filler membranes. For example, PVF and PTFE membranes are well suited to filtering organic solvents while aqueous solutions are filtered through PVF or MCE membranes.
- MCE mixed cellulosic esters
- PVDF polyvirtylidene fluoride
- PTFE polyletrafluoroethylene
- Filter apparatus are available for use on many scales ranging from the single point-of- ⁇ se disposable filter attached to a syringe up to commercial scale filters for use in manufacturing plants.
- the membrane filters are sterilized by autoclave or chemical sterilization. Validation of membrane filtration systems is performed following standardized protocols (Microbiological Evaluation of Filters for Sterilizing Liquids, VoI 4, No. 3. Washington, D.C: Health Industry Manufacturers Association, 1981) and involve challenging the membrane filter with a known quantity (ca. lO' cm 2 ) of unusually small microorganisms, such as Brevundimonas diminuta (ATCC 19146).
- compositions are optionally sterilized by passing through membrane filters.
- Formulations comprising nanoparticles (U.S. Pat No. 6, 139,870) or multilamellar vesicles (Richard et al, International Journal of Pharmaceutics (2006), 312(1 -2): 144-50) are amenable to sterilization by filtration through 0.22 ⁇ m filters without destroying their organized structure.
- the methods disclosed herein comprise sterilizing the formulation (or components thereof) by means of filtration sterilization.
- the auns-acceptable otic therapeutic agent formulation comprises a particle wherein the particle formulation is suitable for filtration sterilization.
- said particle formulation comprises particles of less than 300 nm in size, ofless than 200 am in size, of less than 100 nm in size.
- the auris-acceptable formulation comprises a particle formulation wherein the sterility of the particle is ensured by sterile filtration of the precursor component solutions.
- the auris-acceptable formulation comprises a particle formulation wherein the sterility of the particle formulation is ensured by low temperature sterile filtration.
- said low temperature sterile filtration occurs at a temperature between 0 and 30 °C, or between 0 and 20 °C. or between 0 and 10 °C, or between 10 and 20 °C, or between 20 and 30 °C.
- a process for the preparation of an auris-acceptable particle formulation comprising: filtering the aqueous solution containing the particle formulation at low temperature through a sterilization filter: lyophHizing the ste ⁇ le solution; and reconstituting the particle formulation with sterile water prior to administration.
- filtration and/or filling procedures are carried out at about 5°C below the gel temperature (Tgel) of a formulation described herein and with viscosity below a theoretical value of 1 OOcP to allow for filtration in a reasonable time using a peristaltic pump.
- Tgel gel temperature
- the auris-acceptable otic therapeutic agent formulation comprises a nanoparticle formulation wherein the nanopariicle formulation is suitable for filtration sterilization.
- the nanoparticle formulation comprises nanoparticles ofless than 300 nm in size, ofless than 200 nm. in size, or ofless than 100 nm in sue.
- the auris- acceptable formulation comprises a microsphere formulation wherein the sterility of the microsphere is ensured by sterile filtration of the precursor organic solution and aqueous solutions.
- the auris-acceptable formulation comprises a thermoreversible gel formulation wherein the sterility of the gel formulation is ensured by low temperature sterile filtration.
- the low temperature sterile filtration occurs at a temperature between 0 and 30 °C, or between 0 and 20 °C, or between 0 and 10 °C, or between 10 and 20 °C, or between 20 and 30 °C.
- a process for the preparation of an auris-acceptable thermoreversible gel formulation comprising: filtering the aqueous solution containing the t ⁇ ermoreversible gel components at low temperature through a sterilization filter; lyophilizing the sterile solution; and reconstituting the thermoreversible gel formulation with sterile water prior to administration.
- the active ingredients are dissolved in a suitable vehicle (e.g. a buffer) and sterilized separately (e.g. by heat treatment, filiation, gamma radiation); the remaining excipients (e.g., fluid gel components present in auris formulations) are sterilized in a separate step by a suitable method (e.g. filtration and/or irradiation of a cooled mixture of excipients); the two solutions that were separately sterilized are then mixed aseptically to provide a final auris formulation.
- a suitable vehicle e.g. a buffer
- sterilized separately e.g. by heat treatment, filiation, gamma radiation
- the remaining excipients e.g., fluid gel components present in auris formulations
- a suitable method e.g. filtration and/or irradiation of a cooled mixture of excipients
- sle ⁇ ligation of au ⁇ s formulations that prevent degradation of polymeric components (e.g.. thermosetting and/or gelling and/or mucoadhesive polymer components) and/or the active agent during the process of sterilization.
- degradation of the active agent e.g., any therapeutic otic agent described herein
- the choice of an appropriate gellling agent and/or thermosetting polymer allows for sterilization of formulations described herein by filtration.
- an appropriate thermosetting polymer and an appropriale copolymer e.g., a gellling agent
- a specific pH range for the formulation allows for high temperature sterilization of formulations described with substantially no degradation of the therapeutic agent or the polymeric excipients.
- An advantage of the methods of sterilization provided herein is that, in certain instances, the formulations are subjected to terminal sterilization via autoclaving without any loss of the active agent and/or excipients and/or polymeric components during the sterilization step and are rendered substantially free of microbes and/or pyrogens.
- auris-acceptable compositions that ameliorate or lessen otic disorders described herein.
- methods comprising the administration of said otic compositions.
- the compositions are substantially free of microorganisms.
- Acceptable sterility levels are based on applicable standards that define therapeutically acceptable otic compositions, including but not limited to United States Pharmacopeia Chapters ⁇ 1111> et seq.
- acceptable sterility levels include 10 colony forming units (cfu) per gram of formulation, 50 cfu per gram of formulation. 100 cfu per gram of formulation, 500 cfu per gram of formulation or 1000 cfu per gram of formulation.
- acceptable sterility levels include the exclusion of specified objectionable microbiological agents.
- specified objectionable microbiological agents include but are not limited to Escherichia coli (E. coli), Salmonella sp., Pseudomonas aeruginosa (P. aeruginosa) and/or other specific microbial agents.
- Sterility of the auris-acceptable otic therapeutic agent formulation is confirmed through a sterility assurance program in accordance with United States Pharmacopeia Chapters ⁇ 61 >, ⁇ 62> and ⁇ 71>.
- a key component of the sterility assurance quality control, quality assurance and validation process is the method of sterility testing. Sterility testing, by way of example only, is performed by two methods. The first is direct inoculation wherein a sample of the composition to be tested is added to growth medium and incubated for a period of time up to 21 days. Turbidity of the growth medium indicates contamination. Drawbacks to this method include the small sampling size of bulk materials which reduces sensitivity, and detection of microorganism growth based on a visual observation.
- An alternative method is membrane filtration sterility testing.
- a volume of product is passed through a small membrane filter paper.
- the filter paper is then placed into media to promote the growth of microorganisms.
- This method has the advantage of greater sensitivity as the entire bulk product is sampled.
- the commercially available Millipore Steritest sterility testing system is optionally used for determinations by membrane filtration sterility testing.
- Steritest filter system No. TLHVSL210 are used.
- Steritest filter system No. TLAREM210 or TD AREM210 are used.
- TI ⁇ ASY210 are used.
- material dispensed as an aerosol or foam Steritest filter system No. TTHVA210 are used.
- Steritest filter system No. TTHADA210 or TTHADV210 are used.
- Testing for E. coli and Salmonella includes the use of lactose broths incubated at 30 - 35 °C for 24-72 hours, incubation in MacConkey and/or EMB agars for 18-24 hours, and/or the use of Rappaport medium.
- Testing for the detection of P. aeruginosa includes the use of NAC agar. United States Pharmacopeia Chapter ⁇ 62> further enumerates testing procedures for specified objectionable microorganisms.
- any controlled release formulation described herein has less than about 60 colony forming units (CFU), less than about 50 colony forming units, less than about 40 colony forming units, or less than about 30 colony fo ⁇ ning units of microbial agents per gram of formulation, in certain embodiments, the otic ibmulations described herein are formulated to be isotonic with the endolymph and/or the perilymph.
- CFU colony forming units
- 50 colony forming units less than about 50 colony forming units
- 40 colony forming units less than about 30 colony fo ⁇ ning units of microbial agents per gram of formulation
- the otic ibmulations described herein are formulated to be isotonic with the endolymph and/or the perilymph.
- Endotoxins Provided herein are otic compositions that ameliorate or lessen otic disorders described herein. Further provided herein are methods comprising the administration of said otic compositions, In some embodiments, the compositions are substantially free of endotoxins.
- An additional aspect of the vSteriiization process is the removal of by-products from the killing of microorganisms
- Pyrogens are endotoxins or exotoxins which induce an immune response.
- An example of an endotoxin is the lipopoiysaccharide (LPS) molecule found in the cell wall of gram-negative bacteria. While sterilization procedures such as autoclaving or treatment with ethylene oxide kill the bacteria, the LPS residue induces a proinflammatory immune response, such as septic shock. Because the molecular size of endotoxins can vary widely, the presence of endotoxins is expressed in '"endotoxin units" (ElF). One EU is equivalent to 100 picograms of E. coli LPS. Humans can develop a response to as little as 5 EU/kg of body weight. The sterility is expressed in any units as recognized in the art.
- otic compositions described herein contain lower endotoxin levels (e.g. ⁇ 4 EU/kg of body weight of a subject) when compared to conventionally acceptable endotoxin levels (e.g., 5 EU/kg of body weight of a subject).
- the auris-acceptable otic therapeutic agent formulation has less than about 5 EU/kg of body weight of a subject.
- the auris-acceptable otic therapeutic agent formulation lias less than about 4 EU/kg of body weight of a subject.
- the auris-acceptable otic therapeutic agent formulation has less than about 3 EU/kg of body weight of a subject.
- the auris-acceptable otic therapeutic agent formulation has less than about 2 EU/kg of body weight of a subject.
- the auris-acceptable otic therapeutic agent formulation has less than about 5 EU/kg of formulation. In other embodiments, the auris-acceptable otic therapeutic agent formulation has less than about 4 EU/kg of formulation. In additional embodiments, the auris- acceptable otic therapeutic agent formulation has less than about 3 EU/kg of formulation. In some embodiments, the auris-acceptable otic therapeutic agent formulation has less than about 5 EU/kg Product. In other embodiments, the auris-acceptable otic therapeutic agent formulation has less than about 1 EU/kg Product. In additional embodiments, the auris-acceptable otic therapeutic agent formulation lias less than about 0.2 EU/kg Product.
- the auris-acceptable otic therapeutic agent formulation has less than about 5 EU/g of unit or Product. In other embodiments, the auris-acceptable otic therapeutic agent formulation has less than about 4 EU/ g of unit or Product. In additional embodiments, the auris-acceptabie otic therapeutic agent formulation has less than about 3 EU/g of unit or Product. In some embodiments, the auris-acccptablc otic therapeutic agent formulation has less than about 5 EU/mg of unit or Product. In other embodiments, the auris- acceptable otic therapeutic agent formulation has less than about 4 EU/ mg of unit or Product.
- the auris-acceptable otic therapeutic agent formulation has less than about 3 EU/mg of unit or Product.
- otic compositions described herein contain from about 1 to about 5 EU/mL of formulation. In certain embodiments, otic compositions described herein contain from about 2 to about 5 EU/mL of formulation, from about 3 to about 5 EU/mL. of formulation, or from about 4 to about 5 EU/mL of formulation.
- otic compositions described herein contain lower endotoxin levels (e.g. ⁇ 0.5 EU/mL of formulation) when compared to conventionally acceptable endotoxin levels (e.g., 0.5 EU/mL of formulation).
- the auris-acceptable otic therapeutic agent formulation has less than about 0.5 EU/mL of formulation. In other embodiments, the auris- acceptable otic therapeutic agent formulation has less than about 0.4 EU/mL of formulation. In additional embodiments, the auris-acceptable otic therapeutic agent formulation has less than about 0.2 EU/mL of formulation.
- Pyrogen detection by way of example only, is performed by several methods. Suitable tests for sterility include tests described in United States Pharmacopoeia (USP) ⁇ 71> Sterility Tests (23rd edition, 1995). The rabbit pyrogen test and the Limulus amebocyte lysate test are both specified in the United States Pharmacopeia Chapters ⁇ 85> and ⁇ 151> (USP23/NF 18, Biological Tests, The United States Pharmacopeial Convention, Rockville, MD, 1995). Alternative pyrogen assays have been developed based upon the monocyte activation-cytokine assay.
- the auris- acceptable otic therapeutic agent formulation is subject to depyrogenation.
- the process for the manufacture of the auris-acceptable otic therapeutic agent formulation comprises testing the formulation for pyrogenicity. m certain embodiments, the formulations described herein are substantially free of pyrogens.
- the main cation present in the endolymph is potassium.
- the endolymph has a high concentration of positively charged amino acids.
- the main cation present in the perilymph is sodium-
- the ionic composition of the endolymph and perilymph regulate the electrochemical impulses of hair cells.
- any change in the ionic balance of the endolymph. or perilymph results in a loss of hearing due to changes in the conduction of electrochemical impulses along otic hair cells, hi some embodiments, a composition disclosed herein does not disrupt the ionic balance of the perilymph.
- a composition disclosed herein has an ionic balance that is the same as or substantially the same as the perilymph.
- a composition disclosed herein does not disrupt the ionic balance of the endolymph.
- a composition disclosed herein has an ionic balance that is the same as or substantially the same as the endolymph.
- an otic formulation described herein is formulated to provide an ionic balance that is compatible with inner ear fluids (i.e., endolymph and/or perilymph).
- the endolymph and the perilymph have a p ⁇ that is close to the physiological p ⁇ l of blood.
- the endolymph has a pH range of about 7.2-7.9; the perilymph has a pH range of about 7.2 - 7.4.
- the in situ pH of the proximal endolymph is about 7.4 while the pH of distal endolymph is about 7.9.
- the pH of a composition described herein is adjusted (e.g., by use of a buffer) to an endolymph-eorapatible pH range of about 7.0 to 8.0, and a preferred pH range of about 7.2 - 7.9.
- the pH of the auris formulations described herein is adjusted (e.g., by use of a buffer) to a perilymph - compatible pH of about 7.0 - 7.6, and a preferred pH range of about 7.2-7.4.
- useful formulations also include one or more pH adjusting agents or buffering agents.
- pH adjusting agents or buffers include, but are not limited to acetate, bicarbonate, ammonium chloride, citrate, phosphate, pharmaceutically acceptable salts thereof and combinations or mixtures thereof.
- one or more buffers when utilized in the formulations of the present disclosure, they are combined, e.g., with a pharmaceutically acceptable vehicle and are present in the final formulation, e.g., in an amount ranging from about 0.1% to about 20%, from about 0.5% to about 10%.
- the amount of buffer included in the gel formulations are an amount such that the pH of the gel formulation does not interfere with the body's natural buffering system. In some embodiments, from about 5 mM to about 200 mM concentration of a buffer is present in the gel formulation. In certain embodiments, from about a 20 mM to about a 100 mM concentration of a buffer is present. In other embodiments, the
- concentration of buffer is such that a pH of the formulation is between 3 and 9, between 5 and 8, or alternatively between 6 and 7. In other embodiments, the pH of the gel formulation is about 7.
- a buffer such as acetate or citrate at slightly acidic pH.
- the buffer is a sodium acetate buffer having a pH of about 4.5 to about 6.5.
- the buffer is a sodium acetate buffer having a pH of about 5.5 to about 6.0.
- the buffer is a sodium acetate buffer having a pH of about 6.0 to about 6.5.
- the buffer is a sodium citrate buffer having a pH of about 5.0 to about 8.0.
- the buffer is a sodium citrate buffer having a pll of about 5.5 to about 7.0.
- the buffer is a sodium citrate buffer having a pH of about 6.0 to about 6.5.
- the concentration of buffer is such that a pH of the formulation is between 6 and 9, between 6 and 8, between 6 and 7.6, between 7 and 8.
- the pH of the gel formulation is about 6.0, about 6.5, about 7 or about 7.5.
- a buffer such as tris(hydroxymethyl)aminomethane, bicarbonate, carbonate or phosphate at slightly basic pH.
- the buffer is a sodium bicarbonate buffer having a pH of about 7.5 Io about 8.5.
- the buffer is a sodium bicarbonate buffer having a pH of about 7.0 to about 8.0.
- the buffer is a sodium bicarbonate buffer having a pH of about 6.5 to about 7.0.
- the buffer is a sodium phosphate dibasic buffer having a pH of about 6.0 to about 9.0. In another embodiment the buffer is a sodium phosphate dibasic buffer having a pH of about 7.0 to about 8.5. In one embodiment the buffer is a sodium phosphate dibasic buffer having a pH of about 7.5 to about 8.0.
- diluents are also used to stabilize compounds because they can provide a more stable environment.
- Salts dissolved in buffered solutions (which also can provide pH control or maintenance) are utilized as diluents in the art, including, but not limited to a phosphate buffered saline solution.
- the pH of a composition described herein is between about between about 6.0 and about 7.6, between 7 and about 7.8. between about 7.0 and about 7.6, between about 7.2 and about 7.6, or between about 7.2 and about 7.4. In certain embodiments the pH of a composition described herein is about about 6.0, about 6.5, about 7,0, about 7.1, about 7.2, about 7.3, about 7.4, about 7.5, or about 7.6. In some embodiments, the pH of any formulation described herein is designed to be compatible with the targeted otic structure (e.g., endolymph. perilymph or the like).
- the targeted otic structure e.g., endolymph. perilymph or the like.
- any gel formulation described herein has a pH that allows for sterilization (e.g, by filtration or aseptic mixing or heal treatment and/or autoclaving (e.g., terminal sterilization)) of a gel formulation without degradation of the otic agent or the polymers comprising the gel.
- the buffer pH is designed to maintain pH of the formulation in the 7-8 range during the process of sterilization.
- any gel formulation described herein has a pli that allows for terminal sterilization (e.g, by heat treatment and/or autoclaving) of a gel formulation without degradation of the otic agent or the polymers comprising the gel.
- the buffer pH is designed to maintain pH of the formulation in the 7-8 range at elevated temperatures. Any appropriate buffer is used depending on the otic agent used in the formulation.
- a pH of between between about 6.0 and about 7.6, between about 7 and about 7.8, between about 7.0 and about 7.6, between about 7.2 and 7.6, between about 7.2 and about 7.4 is suitable for sterilization (e.g, by filtration or aseptic mixing or heat treatment and/or autoclaving (e.g., terminal sterilization)) of auris formulations described herein.
- a formulation pH of about 6.0 is suitable for sterilization (e.g, by filtration or aseptic mixing or heat treatment and/or autoclaving (e.g., terminal sterilization)) of auris formulations described herein.
- a formulation pH of about 6.0 is suitable for sterilization (e.g, by filtration or aseptic mixing or heat treatment and/or autoclaving (e.g., terminal sterilization)) of auris formulations described herein.
- a formulation pH of about 6.0 is suitable for sterilization (e.g, by filtration or aseptic mixing or heat treatment and/or autoclaving (e.g., terminal sterilization))
- 6.5, about 7.0, about 7.1 , about 7.2, about 7.3, about 7.4, about 7.5, or about 7.6 is suitable for sterilization (e.g, by filtration or aseptic mixing or heat treatment and/or autoclaving (e.g., terminal sterilization)) of any composition descibed herein.
- the formulations described herein have a pH between about 3 and about 9, or between about 4 and 8, or between about 5 and 8, or between about 6 and about 7, or between about 6.5 and about 7, or between about 5.5 and about 7.5, or between about 7.1 and about 7.7, and have a concentration of active pharmaceutical ingredient between about 0.1 mM and about 100 mM. In some embodiments, the formulations described herein have a pH between about 5 and about 8, or between about 6 and about 7, or between about 6.5 and about 7, or between about 5.5 and about 7.5, or between about 7.1 and about 7.7, and have a concentration of active
- the formulations described herein have a pH between about 5 and about 8, or between about 6 and about 7, or between about 6.5 and about 7, or between about 5.5 and about 7.5, or between about 7.1 and about 7.7, and have a concentration of active pharmaceutical ingredient between about 50 and about 80 mM. In some embodiments, the concentration of active pharmaceutical ingredient hetween about 10 and about 100 mM. In other embodiments, the concentration of active pharmaceutical ingredient between about 20 and about 80 mM. In additional embodiments, the concentration of active pharmaceutical ingredient between about 10 and about 50 mM.
- the formulations have a pH as described herein, and include a thickening agent (i.e, a vicosity enhancing agent) such as, by way of non-limiting example, a cellulose based thickening agent described herein.
- a thickening agent i.e, a vicosity enhancing agent
- a secondary polymer e.g., a thickening agent
- a pH of formulation as described herein allows for sterilization of a formulation described herein without any substantial degradation of the otic agent and/or the polymer components in the otic formulation.
- the ratio of a thermoreversible poloxamer to a thickening agent in a formulation that has a pH as described herein is about 40:1 , about 35:1, about 30:1, about 25: 1, about 20:1, about 15:1 or about 10:1.
- a sustained and/or extended release formulation described herein comprises a combination of poloxamer 407 (pluronic Fl 27) and carboxymethylcellulose (CMC) in a ratio of about 40:1 , about 35: 1, about 30: 1. about 25:1, about 20:1, about 15: 1 or about 10:1.
- the amount of thermoreversible polymer in any formulation described herein is about 10%, about 15%, about 20%, about 25%, about 30%, or about 35% of the total weight of the formulation. In some embodiments, the amount of thermoreversible polymer in any formulation described herein is about 14%. about 15%, about 16%, about 17%, about 18%, about 19%, about 20%, about 21%, about 22%, about 23%, about 24% or about 25% of the total weight of the formulation, In some embodiments, the amount of thickening agent (e.g., a gelling agent.) in any formulation described herein is about 1%, 5%, about 10%, or about 15% of the total weight of the formulation.
- the amount of thickening agent e.g., a gelling agent.
- the amount of thickening agent (e.g., a gelling agent) in any formulation described herein is about 0.5%, about 1%, about 1.5%, about 2%, about 2.5%, about 3%, about 3.5%, about 4%, about 4.5%, or about 5% of the total weight of the formulation.
- the pharmaceutical formulations described herein are stable with respect to pM over a period of any of at least about 1 day, at least about 2 days, at least about 3 days, at least about 4 days, at least about 5 days, at least about 6 days, at ⁇ east about 1 week, at least about 2 weeks, at least about 3 weeks, at least about 4 weeks, at least about 5 weeks, at least about 6 weeks, at least about 7 weeks, at least about 8 weeks, at least about 1 month, at least about 2 months, at least about 3 months, at least about 4 months, at least about 5 months, or at ieast about 6 months.
- the formulations described herein are stable with respect to pH over a period of at least about 1 week. Also described herein are formulations that are stable with respect to pH over a period of at least about 1 month.
- the endolymph has a higher osmolality than the perilymph.
- the endolymph has an osmolality of about 304 m ⁇ sm/kg HjO while the perilymph has an osmolality of about 294 mOsm/kg HjO.
- auris compositions described herein are formulated to provide an osmoiarity of about 250 to about 320 mM (osmolality of about 250 Io about 320 m ⁇ sm/kg EbO) ; and preferably about 270 to about 320 mM (osmolality of about 270 to about 320 mOsm/kg H 2 O ).
- osmolarity/osmolality of the present formulations is adjusted, for example, by the use of appropriate salt concentrations (e.g., concentration of potassium salts) or the use of tonicity agents which renders the formulations endolytnph-compatible an ⁇ Vor perilymph-compatible (i.e. isotonic with the endolymph and/or perilymph.
- appropriate salt concentrations e.g., concentration of potassium salts
- tonicity agents which renders the formulations endolytnph-compatible an ⁇ Vor perilymph-compatible (i.e. isotonic with the endolymph and/or perilymph.
- the endolymph-compatible and/or perilymph-compatible formulations described herein cause minimal disturbance to the environment of the inner ear and cause minimum discomfort (e.g., vertigo and/or nausea) to a mammal upon administration.
- any formulation described herein is isotonic with the perilymph.
- Isotonic formulations are provided by the addition of a tonicity agent.
- Suitable tonicity agents include, but are not limited to any pharmaceutically acceptable sugar, salt or any combinations or mixtures thereof, such as, but not limited to dextrose, glycerin, maimitol, sorbitol, sodium chloride, and other electrolytes.
- Useful auris compositions include one or more salts in an amount required to bring osmolality of the composition into an acceptable range.
- Such salts include those having sodium, potassium or ammonium cations and chloride, citrate, ascorbate, borate, phosphate, bicarbonate, sulfate, thiosuifate or bisulfite anions; suitable salts include sodium chloride, potassium chloride, sodium thiosuifate, sodium bisulfite and ammonium sulfate.
- the tonicity agents are present in an amount as io provide a final osmolality of an otic formulation of about 100 mOsm/kg to about 500 mOsm/kg, from about 200 m ⁇ sra/kg to about 400 mOsm/kg, from about 250 mOsm/kg to about 350 mOsm/kg or from about 280 mOsm/kg to about 320 mOsm/kg.
- the formulations described herein have a osmolality of about 100 m ⁇ sm/l. to about 500 mOsm/L.
- the osmolarity of any formulation described herein is designed to be isotonic with the targeted otic structure (e.g., endolymph, perilymph or the like).
- the formulations described herein have a pH and osmolarity as described herein, and have a concentration of active pliarmaceutical ingredient between about 1 ⁇ M and about 10 ⁇ M, between about 1 mM and about 100 mM, between about 0.1 xnM and about 100 mM, betwen about 0.1 mM and about 100 nM.
- the formulations described herein have a pH and osmolarity as described herein, and have a concentration of active
- the formulations described herein have a pH and osmolarity as described herein, and have a concentration of active pharmaceutical ingredient between about 0.1 ⁇ • about 70 mg/mL, between about I mg ⁇ about 70 mg/mL, between about 1 rag ⁇ • about 50 mg/mL,., between about 1 mg/mL and about 20 mg/mL, between about 1 mg/mL to about 10 mg/mL, between about 1 mg/mL to about 5 mg/mL, or between about 0.5 mg/mL to about 5 mg/mL of the active agent by volume of the formulation.
- Size reduction is used to increase surface area and/or modulate formulation dissolution properties. Tt is also used to maintain a consistent average particle size distribution (PSD) (e.g.. micrometer-sized particles, nanometer-sized particles or the like) for any formulation described herein.
- PSD average particle size distribution
- any formulation described herein comprises mulitparticulai.es, i.e., a plurality of particle sizes (e.g., micronized particles, nano-sized particles, non-sized particles); i.e, the formulation is a multiparticulate formulation.
- any formulation described herein comprises one or more multiparticulate (e.g., micronized) therapeutic agents. Micronization is a process of reducing the average diameter of particles of a solid material.
- Micronized particles are from about micrometer-sized in diameter to about picometer -sized in diameter.
- the use of multiparticulates (e.g., micronized particles) of an otic agent allows for extended and/or sustained release of the otic agent from any formulation described herein compared to a formulation comprising non-multiparticulate (e.g, non-micronized) otic agent.
- formulations containing multiparticulate (e.g. micronized) otic agents are ejected from a I mL syringe adapted with a 27 ⁇ j needle without any plugging or clogging.
- any particle in any formulation described herein is a coated particle (e.g., a coated micronized particle) and/or a microsphere and/or a liposomal particle.
- Particle size reduction techniques include, by way of example, grinding, milling (e.g., air-attrition milling (jet milling), ball milling), coacervation, high pressure homogenization, spray drying and/or supercritical fluid crystallization.
- particles are sized by mechanical impact (e.g., by hammer mills, ball mill and/or pin mills).
- particles are sized via fluid energy (e.g., by spiral jet mills, loop jet mills, and/or fluidized bed jet mills).
- formulations described herein comprise crystalline particles. In some embodiments, formulations described herein comprise amorphous particles. In some embodiments, formulations described herein comprise therapeutic agent particles wherein the therapeutic agent is a free base, or a salt, or a prodrug of a therapeutic agent, or any combination thereof.
- a combination of an otic agent and a salt of the otic agent is used to prepare pulsed release otic agent formulations using the procedures described herein.
- a combination of a micronized otic agent (and/or salt or prodrug thereof) and coated particles is used to prepare pulsed release otic agent formulations using any procedure described herein.
- a pulsed release profile is achieved by solubilizing up to 20% of the delivered dose of the otic agent (e.g., micronized otic agent, or free base or salt or prodrug thereof; multiparticulate otic agent, or free base or salt or prodrug thereof) with the aid of cyclodextrms, surfactants (e.g., poloxamers (407, 338, 188), tween (80, 60, 20,81 ), PEG-hydrogenated castor oil, cosolvents like N-methyl-2-Pyrrolidone or the like and preparing pulsed release formulations using any procedure described herein.
- the otic agent e.g., micronized otic agent, or free base or salt or prodrug thereof; multiparticulate otic agent, or free base or salt or prodrug thereof
- surfactants e.g., poloxamers (407, 338, 188), tween (80, 60, 20,81 ), PEG-hydrogenated castor
- any otic formulation described herein comprises one or more micronized otic agents.
- a micronized otic agent comprises micronized particles, coated (e.g., with an extended release coat) micronized particles, or a combination thereof.
- a micronized otic agent comprising micronized particles, coated micronized particles, or a combination thereof comprises an otic agent as a free base, a salt, a prodrug or any combination thereof.
- any controlled release otic formulation described herein increases the exposure of an otic agent and increases the Area Under the Curve (AUC) in otic fluids (e.g., endolymph and/or perilymph) by about 30%, about 40%, about 50%, about 60%, about 70%, about 80% or about 90% compared to a formulation that is not a controlled release otic formulation
- AUC Area Under the Curve
- any controlled release otic formulation described herein increases the exposure of an otic agent and decreases the C ms ⁇ in otic fluids (e.g., endolymph and/or perilymph) by about 40%, about 30%, about 20%, or about 10%, compared to a formulation that is not a controlled release otic formulation.
- any controlled release otic formulation described herein alters (e.g. reduces) the ratio of C m3x to C m j n compared to a formulation that is not a controlled release otic formulation.
- any controlled release otic formulation described herein increases the exposure of an otic agent and increases the length of time that the concentration of an otic agent is above C, ⁇ by about 30%, about 40%, about 50%, about 60%, about 70%, about 80% or about 90% compared to a formulation that is not a controlled release otic formulation.
- controlled release formulations described herein delay the time to C u )_ x -
- auris compositions described herein prolong the residence time of a drug in the inner ear.
- the concentration of the drug in the endolymph or perilymph stays at or about the therapeutic dose tor an extended period of time (e.g., one day, 2 days, 3 days, 4 days, 5 days, 6 days, or 1 week).
- otic formulations described herein deliver an active agent to the external, middle and/or inner ear, including the cochlea and vestibular labyrinth. Local otic delivery of the auris
- compositions described herein allows for controlled release of active agents to auris structures and overcomes the drawbacks associated with systemic administration (e.g, low bioavailability of the drug in the endolymph or perilymph, variability in concentration of the drug in the middle and/or internal ear).
- Controlled-release options include gel formulations, liposomes, cyciodextrins,
- biodegradable polymers dispersable polymners, emulsions, microspheres or microparticles, hydrogels (e.g., a self-assembling hydrogel displaying thixotropic properties that also functions as an absorption enhancer; including instances in which the penetration enhancer is a surfactant comprising an alkyl -glycoside and/or a saccharide alkyl ester), other viscous media, paints, foams, in situ forming spongy materials, xerogels, actinic radiation curable gels, liposomes, solvent release gels, nanocapsules or nanospheres.
- hydrogels e.g., a self-assembling hydrogel displaying thixotropic properties that also functions as an absorption enhancer; including instances in which the penetration enhancer is a surfactant comprising an alkyl -glycoside and/or a saccharide alkyl ester
- other viscous media paints, foams, in situ forming spong
- thermoreversible gels or post-administration viscosity-enhancing options are also envisioned, as well as alternative delivery systems, including pumps, microinjection devices and the like.
- the aural pressure modulator is provided in a gel formulation, also referred to herein as "auris acceptable gel formulations," “auris i ⁇ tema-acceptable gel formulations,” “auris gel formulations” or variations thereof. All of the components of the gei formulation must be compatible with the auris interna. Further, the gel formulations provide controlled release of the aural pressure modulator to the desired site within the auris interna; in some embodiments, the gel formulation also has an immediate or rapid release component for delivery of the aural pressure modulator to the desired target site.
- auris formulations that comprise
- the formulations are liquid at or below room temperature but gel at body temperatures
- intratympanic injection of cold formulations e.g., formulation with temperatures of ⁇ 20 °C
- cold formulations e.g., formulation with temperatures of ⁇ 20 °C
- the formulations described herein are designed to be liquids that are administered at or near room temperature and do not cause vertigo or other discomfort when administered to an indivdual or patient.
- the formulations are bimodal formulations and comprise an immediate release component and an extended release component.
- bimodal formulations allow for a constant rate of release of an immediate release component
- the otic compositions described herein are administered as a controlled release formulation, released either continuously or in a pulsatile manner, or variants of both.
- the active agent formulation is administered as both an immediate release and controlled release formulation, released either continuously or in a pulsatile manner, or variants of both.
- the formulations comprise penetration enhancers that allow for delivery of the active agents across the oval window or the round window of the ear.
Abstract
Description








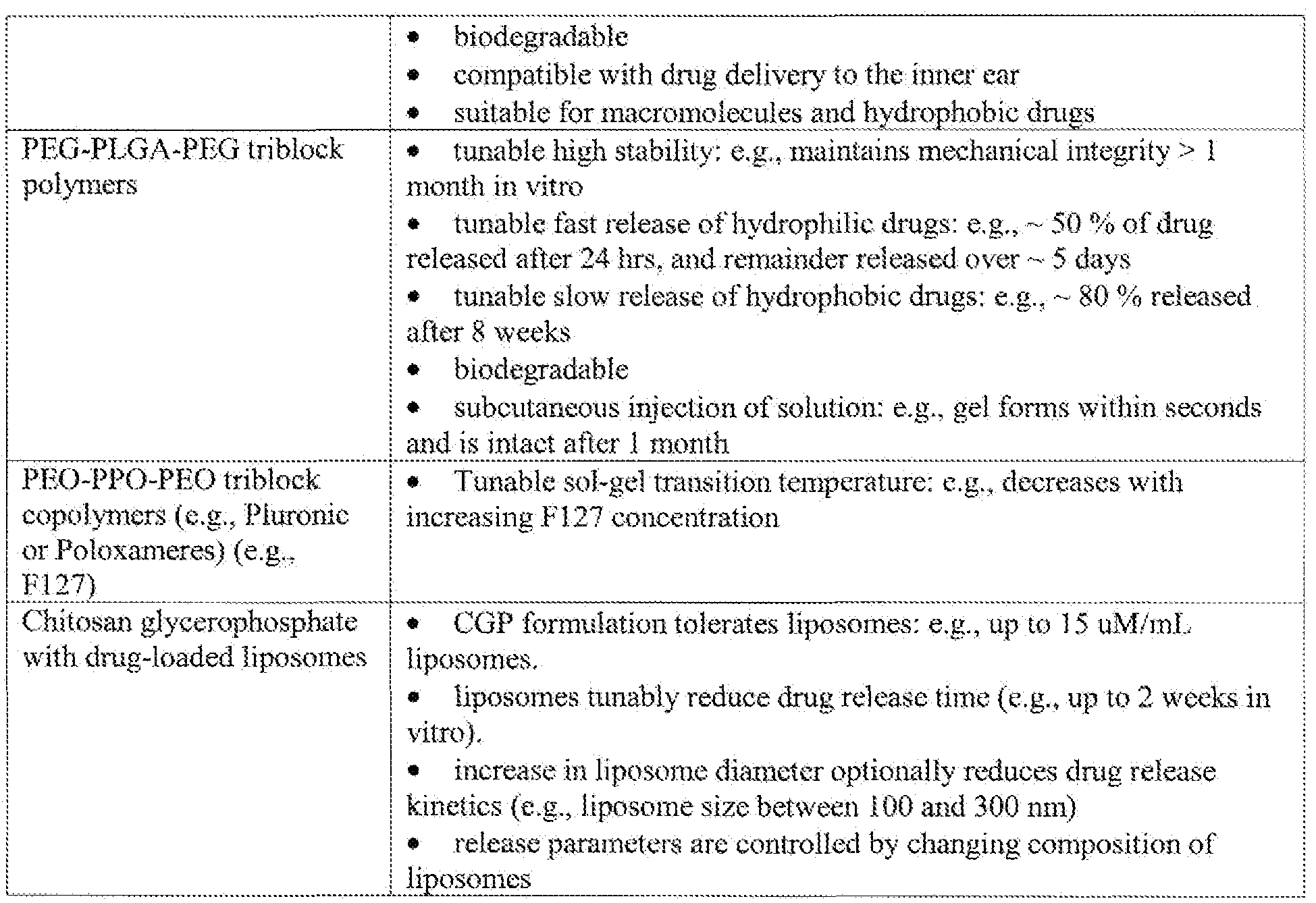




























Claims
Priority Applications (17)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| KR1020197006299A KR20190026056A (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| CN200980114124.XA CN102014957B (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| KR1020107026019A KR101449785B1 (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| EP09734483.2A EP2278999A4 (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| KR1020167005563A KR20160029870A (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| KR1020137020483A KR20130097813A (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| BRPI0910850-5A BRPI0910850B1 (en) | 2008-04-21 | 2009-04-21 | INTRATYMPANIC COMPOSITION INCLUDING BRAIN-DERIVED NEUROTROPHIC GROWTH FACTOR (BDNF) FOR THE TREATMENT OR PREVENTION OF HEARING LOSS |
| KR1020207009042A KR102340754B1 (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| RU2010147298/15A RU2499592C2 (en) | 2008-04-21 | 2009-04-21 | Pharmaceutical composition for treating ear diseases |
| KR1020217026035A KR20210107137A (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| CA2721927A CA2721927C (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| MX2010011545A MX2010011545A (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions. |
| AU2009239429A AU2009239429B2 (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
| JP2011505264A JP2011518195A (en) | 2008-04-21 | 2009-04-21 | Ear formulations and related applications to treat ear diseases and disorders |
| ZA2010/07001A ZA201007001B (en) | 2008-04-21 | 2010-10-01 | Auris formulations for treating otic diseases and conditions |
| IL208549A IL208549A (en) | 2008-04-21 | 2010-10-07 | Auris formulations for treating otic diseases and conditions |
| IL251768A IL251768B (en) | 2008-04-21 | 2017-04-18 | Auris formulations for treating otic diseases and conditions |
Applications Claiming Priority (42)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US4654308P | 2008-04-21 | 2008-04-21 | |
| US61/046,543 | 2008-04-21 | ||
| US4887808P | 2008-04-29 | 2008-04-29 | |
| US61/048,878 | 2008-04-29 | ||
| US12771308P | 2008-05-14 | 2008-05-14 | |
| US61/127,713 | 2008-05-14 | ||
| US5562508P | 2008-05-23 | 2008-05-23 | |
| US61/055,625 | 2008-05-23 | ||
| US6042508P | 2008-06-10 | 2008-06-10 | |
| US61/060,425 | 2008-06-10 | ||
| US7371608P | 2008-06-18 | 2008-06-18 | |
| US61/073,716 | 2008-06-18 | ||
| US7458308P | 2008-06-20 | 2008-06-20 | |
| US61/074,583 | 2008-06-20 | ||
| US7656708P | 2008-06-27 | 2008-06-27 | |
| US7657608P | 2008-06-27 | 2008-06-27 | |
| US61/076,576 | 2008-06-27 | ||
| US61/076,567 | 2008-06-27 | ||
| US8245008P | 2008-07-21 | 2008-07-21 | |
| US61/082,450 | 2008-07-21 | ||
| US8383008P | 2008-07-25 | 2008-07-25 | |
| US8387108P | 2008-07-25 | 2008-07-25 | |
| US61/083,830 | 2008-07-25 | ||
| US61/083,871 | 2008-07-25 | ||
| US8610508P | 2008-08-04 | 2008-08-04 | |
| US8609408P | 2008-08-04 | 2008-08-04 | |
| US61/086,094 | 2008-08-04 | ||
| US61/086,105 | 2008-08-04 | ||
| US8790508P | 2008-08-11 | 2008-08-11 | |
| US8795108P | 2008-08-11 | 2008-08-11 | |
| US61/087,905 | 2008-08-11 | ||
| US61/087,951 | 2008-08-11 | ||
| US8827508P | 2008-08-12 | 2008-08-12 | |
| US61/088,275 | 2008-08-12 | ||
| US9438408P | 2008-09-04 | 2008-09-04 | |
| US61/094,384 | 2008-09-04 | ||
| US10111208P | 2008-09-29 | 2008-09-29 | |
| US61/101,112 | 2008-09-29 | ||
| US14003308P | 2008-12-22 | 2008-12-22 | |
| US61/140,033 | 2008-12-22 | ||
| US16023309P | 2009-03-13 | 2009-03-13 | |
| US61/160,233 | 2009-03-13 |
Publications (3)
| Publication Number | Publication Date |
|---|---|
| WO2009132050A2 WO2009132050A2 (en) | 2009-10-29 |
| WO2009132050A3 WO2009132050A3 (en) | 2010-01-14 |
| WO2009132050A9 true WO2009132050A9 (en) | 2011-02-03 |
Family
ID=41217397
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2009/041320 WO2009132050A2 (en) | 2008-04-21 | 2009-04-21 | Auris formulations for treating otic diseases and conditions |
Country Status (13)
| Country | Link |
|---|---|
| US (8) | US9132087B2 (en) |
| EP (1) | EP2278999A4 (en) |
| JP (6) | JP2011518195A (en) |
| KR (6) | KR20190026056A (en) |
| CN (2) | CN102014957B (en) |
| AU (1) | AU2009239429B2 (en) |
| BR (1) | BRPI0910850B1 (en) |
| CA (1) | CA2721927C (en) |
| HK (1) | HK1209055A1 (en) |
| IL (2) | IL208549A (en) |
| MX (1) | MX2010011545A (en) |
| RU (1) | RU2499592C2 (en) |
| WO (1) | WO2009132050A2 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11369607B2 (en) | 2014-09-03 | 2022-06-28 | The Brigham And Women's Hospital, Inc. | Compositions, systems, and methods for generating inner ear hair cells for treatment of hearing loss |
Families Citing this family (128)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CA2669693C (en) | 2006-11-15 | 2018-06-12 | Massachusetts Eye & Ear Infirmary | Generation of inner ear cells |
| US9994585B2 (en) | 2007-12-31 | 2018-06-12 | Aphios Corporation | Transplantation therapies |
| AU2009239429B2 (en) | 2008-04-21 | 2013-08-29 | Otonomy, Inc. | Auris formulations for treating otic diseases and conditions |
| JP5551685B2 (en) | 2008-05-14 | 2014-07-16 | オトノミ―,インク. | Controlled release corticosteroid compositions and methods of treating otic disorders |
| US8846770B2 (en) | 2008-06-18 | 2014-09-30 | Otonomy, Inc. | Controlled release aural pressure modulator compositions and methods for the treatment of OTIC disorders |
| GB2461962B (en) * | 2008-07-25 | 2011-02-16 | Otonomy Inc | Slow release NMDA receptor antagonist for otic disorders |
| WO2010011466A2 (en) | 2008-06-27 | 2010-01-28 | Otonomy, Inc. | Controlled-release cns modulating compositions and methods for the treatment of otic disorders |
| US8784870B2 (en) | 2008-07-21 | 2014-07-22 | Otonomy, Inc. | Controlled release compositions for modulating free-radical induced damage and methods of use thereof |
| US8496957B2 (en) * | 2008-07-21 | 2013-07-30 | Otonomy, Inc | Controlled release auris sensory cell modulator compositions and methods for the treatment of otic disorders |
| US8318817B2 (en) | 2008-07-21 | 2012-11-27 | Otonomy, Inc. | Controlled release antimicrobial compositions and methods for the treatment of otic disorders |
| CA2733918A1 (en) * | 2008-08-11 | 2010-02-18 | Auckland Uniservices Limited | The treatment of hearing loss |
| JP2012506436A (en) | 2008-10-22 | 2012-03-15 | ハウス イアー インスティトゥート | Treatment and / or prevention of inner ear diseases by modulation of metabotropic glutamate receptors |
| US8987328B2 (en) * | 2008-10-30 | 2015-03-24 | Trinity Laboratories, Inc. | Esters of capsaicinoids as dietary supplements |
| WO2010060088A2 (en) | 2008-11-24 | 2010-05-27 | Massachusetts Eye & Ear Infirmary | Pathways to generate hair cells |
| JP6013736B2 (en) * | 2008-12-22 | 2016-10-25 | オトノミ—,インク. | Controlled release of an ear sensory cell modulator composition for the treatment of otic disorders and methods thereof |
| JP5797191B2 (en) | 2009-06-05 | 2015-10-21 | 13セラピューティクス, インコーポレイテッド | Immunomodulating peptides and uses thereof |
| ES2563777T3 (en) | 2009-08-24 | 2016-03-16 | Hough Ear Institute | Nitrona compounds to treat sensorineural hearing loss |
| JP2013503166A (en) * | 2009-08-25 | 2013-01-31 | カーディオカイン・バイオファーマ・エルエルシー | Composition for delivering an insoluble agent |
| US20140076336A1 (en) * | 2009-09-17 | 2014-03-20 | Ascentia Health, Inc. | Ear insert for relief of tmj discomfort and headaches |
| EP3508197A1 (en) * | 2009-10-21 | 2019-07-10 | Otonomy, Inc. | Modulation of gel temperature of poloxamer-containing formulations |
| CN102008470B (en) * | 2010-05-24 | 2012-08-29 | 中国人民解放军第二军医大学 | Compound preparation and use thereof for preventing and treating noise induced hearing damage |
| WO2011150859A1 (en) * | 2010-06-04 | 2011-12-08 | Comprehensive Drug Enterprises Ltd | Oral meclizine aqueous formulations with taste flavoring agent |
| WO2011156631A2 (en) * | 2010-06-09 | 2011-12-15 | Joule Unlimited Technologies, Inc. | Methods and compositions to extract carbon-based products from host cells |
| DE102010030053A1 (en) * | 2010-06-14 | 2011-12-15 | Awd.Pharma Gmbh & Co.Kg | Injectable dosage form of flupirtine |
| WO2011157449A1 (en) * | 2010-06-18 | 2011-12-22 | Merz Pharma Gmbh & Co. Kgaa | Gel formulations for the topical use of 1-amino-alkylcyclohexane derivatives |
| KR101134622B1 (en) * | 2010-08-12 | 2012-04-09 | 한국원자력연구원 | Substained release hydrogels comprising amphotericin B and preparation method thereof |
| SG10201507554RA (en) | 2010-09-13 | 2015-10-29 | Bev Rx Inc | Aqueous drug delivery system comprising off - flavor masking agent |
| WO2012112810A1 (en) * | 2011-02-18 | 2012-08-23 | Otonomy, Inc. | Prevention of and recovery from drug-induced ototoxicity |
| JP2014507441A (en) * | 2011-02-25 | 2014-03-27 | エイド・ファルマ | Nano-encapsulation of essential oils to prevent or treat infections alone or with antibiotics |
| US8580748B2 (en) * | 2011-04-06 | 2013-11-12 | 13Therapeutics, Inc. | Peptides for the treatment of hearing |
| CN102805896A (en) * | 2011-05-30 | 2012-12-05 | 惠觅宙 | Transdermal administration method, preparation and system |
| BR112013031402A2 (en) * | 2011-06-07 | 2017-06-27 | Autifony Therapeutics Ltd | hydantoin derivatives as kv3 inhibitors |
| WO2013033513A1 (en) | 2011-08-31 | 2013-03-07 | University Of Georgia Research Foundation, Inc. | Apoptosis-targeting nanoparticles |
| RU2480214C1 (en) | 2011-09-22 | 2013-04-27 | Валентина Ивановна Ахапкина | Formulation possessing modulatory activity with adequate effect, pharmaceutical substance (versions), use of pharmaceutical substance, pharmaceutical and parapharmaceutical composition (versions), method for preparing pharmaceutical formulations |
| US20140341940A1 (en) * | 2011-11-09 | 2014-11-20 | Iseu da Silva Nunes | Immunomodulator for the treatment of cancerous tumors in the epithelial tissue lining surfaces inside or outside body organs |
| WO2013090452A1 (en) * | 2011-12-12 | 2013-06-20 | Orbis Biosciences, Inc. | Sustained release particle formulations |
| US9034347B2 (en) * | 2011-12-19 | 2015-05-19 | Arphios Corporation | Drug delivery system and method for the treatment of neuro-degenerative disease |
| WO2013123298A1 (en) | 2012-02-17 | 2013-08-22 | University Of Georgia Research Foundation, Inc. | Nanoparticles for mitochondrial trafficking of agents |
| WO2013124416A1 (en) * | 2012-02-23 | 2013-08-29 | INSERM (Institut National de la Santé et de la Recherche Médicale) | Calcineurin inhibitors for use in the treatment of lesional vestibular disorders |
| US20150044271A1 (en) | 2012-02-27 | 2015-02-12 | O-Ray Pharma, Inc. | Solid drug implants for intracochlear delivery of therapeutics for the treatment of otic disorders |
| US20130288981A1 (en) * | 2012-04-02 | 2013-10-31 | Buck Institute For Research On Aging | Targeting senescent cells and cancer cells by interference with jnk and/or foxo4 |
| ES2785303T3 (en) * | 2012-07-16 | 2020-10-06 | Univ Cornell | Nicotinamide riboside to treat hearing loss |
| JP2015527398A (en) | 2012-09-07 | 2015-09-17 | マサチューセッツ アイ アンド イヤー インファーマリー | Hearing loss treatment |
| US10828276B2 (en) | 2012-11-28 | 2020-11-10 | Aphios Corporation | Combination therapeutics and methods for the treatment of neurodegenerative and other diseases |
| EP4056677A1 (en) | 2013-03-14 | 2022-09-14 | The Brigham & Women's Hospital, Inc. | Compositions and methods for epithelial stem cell expansion and culture |
| WO2014178892A1 (en) * | 2013-05-03 | 2014-11-06 | Scanlan Thomas S | Use of sobetirome in the treatment of x-linked adrenolenoleukodystrophy |
| ES2811527T3 (en) * | 2013-06-18 | 2021-03-12 | Univ New York | Pharmaceutical compositions containing a mutated leukocidin E |
| CN105682742A (en) | 2013-08-27 | 2016-06-15 | 奥德纳米有限公司 | Treatment of pediatric otic disorders |
| EP2853533A1 (en) * | 2013-09-29 | 2015-04-01 | Audiocure Pharma GmbH | 6-fluor-9-methyl-ß-carbolin |
| RU2551359C9 (en) * | 2013-11-28 | 2021-08-20 | Общество с ограниченной ответственностью "Мамонт Фарм" | Nanosize weakly crystalline modification of 4-methyl-n-[3-(4-methylimidazol-1-yl)-5-(trifluoromethyl)phenyl]-3-[(4-pyridin-3-ylpyrimidin-2-yl)amino]benazamide hydrochloride monohydrate, method for production thereof and pharmaceutical composition based thereon |
| WO2015126192A1 (en) * | 2014-02-20 | 2015-08-27 | 아주대학교산학협력단 | Pharmaceutical composition for treating or preventing sensorineural hearing loss, containing cysteinyl leukotriene receptor antagonist and ginkgo leaf extract |
| US10398663B2 (en) | 2014-03-14 | 2019-09-03 | University Of Georgia Research Foundation, Inc. | Mitochondrial delivery of 3-bromopyruvate |
| CA2945785A1 (en) * | 2014-04-23 | 2015-10-29 | Auris Medical Ag | Methods and compositions for treating and preventing tinnitus |
| US10010585B2 (en) * | 2014-06-16 | 2018-07-03 | Massachusetts Eye And Ear Infirmary | Methods of treating vestibular schwannoma and reducing hearing or neurite loss caused by vestibular schwannoma |
| WO2016022776A2 (en) | 2014-08-06 | 2016-02-11 | Massachusetts Eye And Ear Infirmary | Increasing atoh1 life to drive sensorineural hair cell differentiantion |
| US10058542B1 (en) | 2014-09-12 | 2018-08-28 | Thioredoxin Systems Ab | Composition comprising selenazol or thiazolone derivatives and silver and method of treatment therewith |
| BR112017006778A2 (en) * | 2014-10-01 | 2018-01-09 | Als Mountain Llc | pharmaceutical composition comprising aspirin, metformin and serotonin with nonionic surfactant |
| WO2016134292A1 (en) | 2015-02-20 | 2016-08-25 | Oregon Health & Science University | Derivatives of sobetirome |
| KR101636733B1 (en) * | 2015-02-24 | 2016-07-07 | 인제대학교 산학협력단 | Health food composition for enhancing exercise ability comprising echinochrome A and method for enhancing exercise ability using the same |
| EP3328898B8 (en) * | 2015-07-28 | 2024-04-10 | 6452728 Canada Corp. | Trkb or trkc agonist compositions and methods for the treatment of otic conditions |
| EP3368553B1 (en) * | 2015-10-27 | 2023-08-02 | Purdue Research Foundation | Polymer-based therapeutics for inductive browning of fat |
| EP3373907A4 (en) * | 2015-11-11 | 2019-12-18 | Qrono, Inc. | Sustained release pharmaceutical compositions and methods of use |
| HRP20231453T1 (en) | 2015-11-16 | 2024-03-01 | Medincell S.A. | A method for morselizing and/or targeting pharmaceutically active principles to synovial tissue |
| US11185536B2 (en) | 2015-12-04 | 2021-11-30 | Massachusetts Eye And Ear Infirmary | Treatment of hearing loss by inhibition of casein kinase 1 |
| EP3400286A1 (en) | 2016-01-08 | 2018-11-14 | Massachusetts Institute Of Technology | Production of differentiated enteroendocrine cells and insulin producing cells |
| WO2017132530A1 (en) | 2016-01-29 | 2017-08-03 | Massachusetts Eye And Ear Infirmary | Expansion and differentiation of inner ear supporting cells and methods of use thereof |
| US10772563B2 (en) * | 2016-02-26 | 2020-09-15 | Med-El Elektromedizinische Geraete Gmbh | Detection of electrically evoked stapedius reflex |
| US11260130B2 (en) | 2016-03-02 | 2022-03-01 | Frequency Therapeutics, Inc. | Solubilized compositions for controlled proliferation of stem cells / generating inner ear hair cells using a GSK3 inhibitor: IV |
| US10213511B2 (en) | 2016-03-02 | 2019-02-26 | Frequency Therapeutics, Inc. | Thermoreversible compositions for administration of therapeutic agents |
| US10201540B2 (en) | 2016-03-02 | 2019-02-12 | Frequency Therapeutics, Inc. | Solubilized compositions for controlled proliferation of stem cells / generating inner ear hair cells using GSK3 inhibitors: I |
| KR101785455B1 (en) * | 2016-03-16 | 2017-11-20 | 전남대학교산학협력단 | A pharmaceutical composition including oat extract as an active ingredient for preventing or treating hearing loss |
| WO2017185061A1 (en) | 2016-04-21 | 2017-10-26 | Astrocyte Pharmaceuticals, Inc. | Compounds and methods for treating neurological and cardiovascular conditions |
| US10821185B2 (en) | 2016-06-29 | 2020-11-03 | Otonomy Inc. | Triglyceride otic formulations and uses thereof |
| WO2018017834A1 (en) * | 2016-07-21 | 2018-01-25 | The Regents Of The University Of California | Methods for inducing stereocilia on hair cells |
| EP3512513A4 (en) | 2016-09-16 | 2020-04-15 | Otonomy, Inc. | Otic gel formulations for treating otitis externa |
| US10707531B1 (en) | 2016-09-27 | 2020-07-07 | New Dominion Enterprises Inc. | All-inorganic solvents for electrolytes |
| JP2019537582A (en) * | 2016-10-31 | 2019-12-26 | ハフ イアー インスティテュート | Methods for enhancing synapse formation and neurite formation |
| US11253193B2 (en) * | 2016-11-08 | 2022-02-22 | Cochlear Limited | Utilization of vocal acoustic biomarkers for assistive listening device utilization |
| US20190321493A1 (en) * | 2016-11-18 | 2019-10-24 | Mayo Foundation For Medical Education And Research | Materials and methods for treating regional pain |
| EP3554487A4 (en) * | 2016-12-13 | 2020-10-21 | The Regents of The University of California | Xenobiotic-free culture system to expand human limbal stem cells |
| RU2630129C1 (en) * | 2016-12-19 | 2017-09-05 | Государственное бюджетное учреждение здравоохранения города Москвы "Научно-исследовательский клинический институт оториноларингологии им. Л.И. Свержевского" Департамента здравоохранения города Москвы | Method for determining level of endolymphatic hydrops in meniere disease, selection of treatment strategy and evaluation of its efficiency |
| CN110392686A (en) | 2016-12-30 | 2019-10-29 | 频率治疗公司 | 1H- pyrrole-2,5-diones compound and making be used to induction it is dry/method of ancestral's sertoli cell self-renewing |
| HUE050829T2 (en) * | 2017-02-02 | 2021-01-28 | Otolanum Ag | Intranasal composition comprising betahistine |
| WO2018195355A1 (en) * | 2017-04-19 | 2018-10-25 | Rxi Pharmaceuticals Corporation | Topical delivery of nucleic acid compounds |
| JP6443783B2 (en) | 2017-06-07 | 2018-12-26 | 株式会社エコ・プランナー | Heat exchange device control method, heat exchange device, and water-cooled heat pump air conditioner |
| US20190054185A1 (en) * | 2017-08-18 | 2019-02-21 | King Fahd University Of Petroleum And Minerals | Use of nano-sized clay crystallites to restore adhesion among tumor and aging stem cells |
| WO2019071245A1 (en) | 2017-10-06 | 2019-04-11 | Foundry Therapeutics, Inc. | Implantable depots for controlled release of analgesics to treat postoperative pain associated with orthopedic surgery, and associated devices, systems, and methods |
| US11484515B2 (en) * | 2017-12-12 | 2022-11-01 | University of Pittsburgh—of the Commonwealth System of Higher Education | Thermoresponsive hydrogel containing polymer microparticles for controlled drug delivery to the ear |
| US11918653B2 (en) * | 2017-12-22 | 2024-03-05 | Dompé Farmaceutici S.P.A. | Triglyceride otic formulations and uses thereof |
| IL275780B1 (en) * | 2018-01-09 | 2024-03-01 | Otonomy Inc | Growth factor otic formulations |
| WO2019152110A1 (en) * | 2018-01-31 | 2019-08-08 | Kci Usa, Inc. | Antimicrobial composition, dressing, dressing components, and method |
| CA3090783A1 (en) | 2018-02-09 | 2019-08-15 | Decibel Therapeutics, Inc. | Hypertonic pharmaceutical compositions containing an anti-platinum chemoprotectant agent |
| US11839615B2 (en) | 2018-02-09 | 2023-12-12 | Astrocyte Pharmaceuticals, Inc. | Compounds and methods for treating addiction and related disorders |
| US11123453B2 (en) * | 2018-02-21 | 2021-09-21 | Shinshu University | Liquid embolic agent composition |
| WO2019195546A1 (en) * | 2018-04-04 | 2019-10-10 | Alivio Therapeutics, Inc. | Self-assembled gels for controlled delivery of biologics and methods of making thereof |
| EP3837351A1 (en) | 2018-08-17 | 2021-06-23 | Frequency Therapeutics, Inc. | Compositions and methods for generating hair cells by downregulating foxo |
| JP2021533788A (en) | 2018-08-17 | 2021-12-09 | フリークエンシー セラピューティクス インコーポレイテッド | Compositions and Methods for Generating Hair Cells by Up-Controlling JAG-1 |
| JP2022502405A (en) | 2018-09-26 | 2022-01-11 | アストロサイト ファーマシューティカルズ, インコーポレイテッド | Polymorphic compounds and their use |
| EP3894383A1 (en) | 2018-12-12 | 2021-10-20 | Autobahn Therapeutics, Inc. | Novel thyromimetics |
| US20210321910A1 (en) * | 2018-12-12 | 2021-10-21 | Takeichi Kanzaki Cabrera | System and Method for Detecting Auditory Biomarkers |
| US10561736B1 (en) | 2019-01-09 | 2020-02-18 | Spiral Therapeutics, Inc. | Apoptosis inhibitor formulations for prevention of hearing loss |
| US11667606B2 (en) | 2019-03-01 | 2023-06-06 | Autobahn Therapeutics, Inc. | Thyromimetics |
| CN114040782A (en) * | 2019-04-30 | 2022-02-11 | 威斯康星州医药大学股份有限公司 | Transtympanic membrane delivery platform and uses thereof |
| CN110101871B (en) * | 2019-05-30 | 2022-03-25 | 广东工业大学 | Preparation method of embedded resveratrol |
| US10813947B1 (en) | 2019-05-31 | 2020-10-27 | Decibel Therapeutics, Inc. | Methods of otoprotection against platinum-based antineoplastic agents |
| WO2020254249A1 (en) * | 2019-06-21 | 2020-12-24 | Proqr Therapeutics Ii B.V. | Delivery of nucleic acids for the treatment of auditory disorders |
| BR112022000445A2 (en) * | 2019-09-24 | 2022-04-19 | Halliburton Energy Services Inc | method and system |
| RU2749857C1 (en) * | 2019-12-23 | 2021-06-17 | Псарева Нелли Александровна | Method for combatting otitis media and otitis externa |
| KR102530724B1 (en) | 2020-01-13 | 2023-05-09 | 아스트로메디컬 바이오테크놀로지, 리미티드 | Use of ketamine in the treatment of cachexia |
| EP3854385A1 (en) * | 2020-01-27 | 2021-07-28 | ROS Therapeutics ApS | Methotrexate dosage form |
| RU2741252C1 (en) * | 2020-06-01 | 2021-01-22 | федеральное государственное автономное образовательное учреждение высшего образования Первый Московский государственный медицинский университет имени И.М. Сеченова Министерства здравоохранения Российской Федерации (Сеченовский университет) (ФГАОУ ВО Первый МГМУ им. И.М. Сеченова Минздрава России (Се | Method for selecting a method of surgical management of patients with meniere's disease |
| CA3189263A1 (en) * | 2020-08-10 | 2022-02-10 | Ziropa, Inc. | Compositions and methods for topical delivery |
| WO2022047234A1 (en) * | 2020-08-28 | 2022-03-03 | President And Fellows Of Harvard College | Drug combination kits and methods of drug delivery |
| RU2751697C1 (en) * | 2020-09-09 | 2021-07-15 | Федеральное государственное бюджетное образовательное учреждение высшего образования "Донской государственный аграрный университет" | Remedy for treatment of otitis of external auditory canal in dogs |
| CN112125969A (en) * | 2020-09-30 | 2020-12-25 | 东南大学 | Application of biological factor RIMBP2 in maintaining inner ear hair cell characteristics |
| CN112618571B (en) * | 2020-09-30 | 2023-04-07 | 杭州贤石生物科技有限公司 | Injectable hydrogel microspheres for treating orthopedic diseases and preparation method and application thereof |
| US20240016766A1 (en) | 2020-11-26 | 2024-01-18 | Alain Moussy | Pharmaceutical composition for treatment of inner ear disorders through local administration in the tympanic area |
| CN112557158B (en) * | 2021-02-28 | 2021-05-28 | 中国工程物理研究院核物理与化学研究所 | Separation, purification and collection device for xenon in air sample |
| CN113425852B (en) * | 2021-05-24 | 2022-06-03 | 北京大学 | Conjugate capable of penetrating blood labyrinth barrier and preparation method thereof |
| CN113456580B (en) * | 2021-07-21 | 2024-03-22 | 沈阳化工大学 | Resveratrol in-situ gel preparation and characterization method thereof |
| KR20230034794A (en) | 2021-09-03 | 2023-03-10 | 충남대학교산학협력단 | Hydrogel composition containing nanoparticles for topical drug delivery for the treatment of inner ear disease |
| WO2023118544A1 (en) * | 2021-12-23 | 2023-06-29 | Cilcare Dev | 4-phenyl-tetrahydropyridine derivatives for treating hearing diseases |
| WO2023154770A1 (en) * | 2022-02-09 | 2023-08-17 | 9 Meters Biopharma, Inc. | Compositions and methods for inhibiting rho kinase |
| WO2023230430A1 (en) * | 2022-05-21 | 2023-11-30 | Neuvision Development Llc | Topical ocular administration of ambroxol for ocular pain |
| EP4299059A1 (en) | 2022-07-01 | 2024-01-03 | Labelic Analysis, S.L. | Composition for the treatment of tinnitus |
| EP4316462A1 (en) * | 2022-08-05 | 2024-02-07 | Dompé farmaceutici S.p.a. | Intranasal administration of bdnf for the treatment of sensorineural hearing loss |
| CN115317446A (en) * | 2022-09-01 | 2022-11-11 | 黑龙江迪龙制药有限公司 | Compound preparation containing gastrodin and preparation method thereof |
| CN116019818B (en) * | 2023-01-18 | 2024-03-19 | 上海交通大学医学院附属第九人民医院 | Composition for preventing, improving and/or treating cochlear synaptic injury and application thereof |
Family Cites Families (190)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US3773919A (en) | 1969-10-23 | 1973-11-20 | Du Pont | Polylactide-drug mixtures |
| DE2010115A1 (en) | 1970-03-04 | 1971-09-16 | Farbenfabriken Bayer Ag, 5090 Leverkusen | Process for the production of micro-granules |
| US4188373A (en) | 1976-02-26 | 1980-02-12 | Cooper Laboratories, Inc. | Clear, water-miscible, liquid pharmaceutical vehicles and compositions which gel at body temperature for drug delivery to mucous membranes |
| US4389330A (en) | 1980-10-06 | 1983-06-21 | Stolle Research And Development Corporation | Microencapsulation process |
| US4675189A (en) | 1980-11-18 | 1987-06-23 | Syntex (U.S.A.) Inc. | Microencapsulation of water soluble active polypeptides |
| US4474572A (en) | 1981-09-29 | 1984-10-02 | Syntex (U.S.A.) Inc. | Implanting device and implant magazine |
| US4530840A (en) | 1982-07-29 | 1985-07-23 | The Stolle Research And Development Corporation | Injectable, long-acting microparticle formulation for the delivery of anti-inflammatory agents |
| US4478822A (en) * | 1983-05-16 | 1984-10-23 | Merck & Co., Inc. | Drug delivery system utilizing thermosetting gels |
| US4968507A (en) * | 1984-06-20 | 1990-11-06 | Merck & Co., Inc. | Controlled porosity osmotic pump |
| US4758435A (en) | 1986-08-11 | 1988-07-19 | American Cyanamid Company | Estradiol implant composition and method for preparation |
| US5052558A (en) | 1987-12-23 | 1991-10-01 | Entravision, Inc. | Packaged pharmaceutical product |
| US5033252A (en) | 1987-12-23 | 1991-07-23 | Entravision, Inc. | Method of packaging and sterilizing a pharmaceutical product |
| US4900552A (en) | 1988-03-30 | 1990-02-13 | Watson Laboratories, Inc. | Mucoadhesive buccal dosage forms |
| US4938763B1 (en) | 1988-10-03 | 1995-07-04 | Atrix Lab Inc | Biodegradable in-situ forming implants and method of producing the same |
| US5702716A (en) | 1988-10-03 | 1997-12-30 | Atrix Laboratories, Inc. | Polymeric compositions useful as controlled release implants |
| US6436425B1 (en) | 1988-11-16 | 2002-08-20 | Mdv Technologies, Inc. | Method and non-gelling composition for inhibiting post-surgical adhesions |
| US5324519A (en) | 1989-07-24 | 1994-06-28 | Atrix Laboratories, Inc. | Biodegradable polymer composition |
| WO1991008231A1 (en) | 1989-11-29 | 1991-06-13 | Brigham And Women's Hospital | [Ala IL-8]77 AS A LEUKOCYTE ADHESION INHIBITOR |
| US5292516A (en) * | 1990-05-01 | 1994-03-08 | Mediventures, Inc. | Body cavity drug delivery with thermoreversible gels containing polyoxyalkylene copolymers |
| US5714167A (en) | 1992-06-15 | 1998-02-03 | Emisphere Technologies, Inc. | Active agent transport systems |
| US6221367B1 (en) | 1992-06-15 | 2001-04-24 | Emisphere Technologies, Inc. | Active agent transport systems |
| IT1251151B (en) * | 1991-08-05 | 1995-05-04 | Fidia Spa | SPONGY MATERIAL ESSENTIALLY CONSTITUTED BY HYALURONIC ACID, OR ITS DERIVATIVES |
| EP0551626A1 (en) | 1991-12-19 | 1993-07-21 | LEK, tovarna farmacevtskih in kemicnih izdelkov, d.d. | Thermoreversible gel as a liquid pharmaceutical carrier for a galenic formulation |
| US5323907A (en) | 1992-06-23 | 1994-06-28 | Multi-Comp, Inc. | Child resistant package assembly for dispensing pharmaceutical medications |
| US6083354A (en) | 1992-07-24 | 2000-07-04 | Matsushita Electric Industrial Co., Ltd. | Treatment method for diamonds |
| US6090925A (en) | 1993-03-09 | 2000-07-18 | Epic Therapeutics, Inc. | Macromolecular microparticles and methods of production and use |
| US5981719A (en) | 1993-03-09 | 1999-11-09 | Epic Therapeutics, Inc. | Macromolecular microparticles and methods of production and use |
| US5578709A (en) | 1993-03-09 | 1996-11-26 | Middlesex Sciences, Inc. | Macromolecular microparticles and methods of production |
| AU7376494A (en) * | 1993-08-04 | 1995-02-28 | Andrulis Pharmaceuticals Corporation | Treatment of rheumatoid arthritis with thalidomide alone or in combination with other anti-inflammatory agents |
| US5421818A (en) | 1993-10-18 | 1995-06-06 | Inner Ear Medical Delivery Systems, Inc. | Multi-functional inner ear treatment and diagnostic system |
| JP4259610B2 (en) | 1994-04-08 | 2009-04-30 | キューエルティー・ユーエスエイ・インコーポレーテッド | Liquid delivery composition |
| TW438601B (en) | 1994-05-18 | 2001-06-07 | Janssen Pharmaceutica Nv | New mucoadhesive emulsion compositions and a process for the preparation thereof |
| WO1996000081A1 (en) | 1994-06-24 | 1996-01-04 | Immunex Corporation | Controlled release polypeptide compositions and methods of treating inflammatory bowel disease |
| GB9505032D0 (en) | 1995-03-13 | 1995-05-03 | Westminster Lab Ltd | Improvements in or relating to organic compositions |
| IL112834A (en) | 1995-03-01 | 2000-12-06 | Yeda Res & Dev | Pharmaceutical compositions for controlled release of soluble receptors |
| JPH11510837A (en) * | 1995-07-28 | 1999-09-21 | フォーカル,インコーポレイテッド | Multi-block biodegradable hydrogels for use as controlled release and tissue treatment agents for drug delivery |
| FR2742357B1 (en) | 1995-12-19 | 1998-01-09 | Rhone Poulenc Rorer Sa | STABILIZED AND FILTRABLE NANOPARTICLES UNDER STERILE CONDITIONS |
| FR2742750B1 (en) | 1995-12-22 | 1998-01-30 | Oreal | NOVEL DERIVATIVES OF L-2-OXOTHIAZOLIDINE 4-CARBOXYLIC ACID AND THEIR USE FOR SKIN CARE |
| US6225282B1 (en) * | 1996-01-05 | 2001-05-01 | Genentech, Inc. | Treatment of hearing impairments |
| US5837681A (en) * | 1996-02-23 | 1998-11-17 | Amgen Inc. | Method for treating sensorineural hearing loss using glial cell line-derived neurotrophic factor (GDNF) protein product |
| US5929041A (en) | 1996-02-23 | 1999-07-27 | Amgen Inc. | Method for preventing and treating sensorineural hearing loss and vestibular disorders using glial cell line-derived neurotrophic factor(GDNF) protein product |
| AU1739097A (en) | 1996-02-23 | 1997-09-10 | Albert Einstein College Of Medicine Of Yeshiva University | Enzyme detection/assay method and substrates |
| WO1997038698A1 (en) | 1996-04-18 | 1997-10-23 | University Technology Corporation | Methods for treating middle and inner ear disorders |
| US5861174A (en) | 1996-07-12 | 1999-01-19 | University Technology Corporation | Temperature sensitive gel for sustained delivery of protein drugs |
| US6156728A (en) * | 1996-11-01 | 2000-12-05 | Genentech, Inc. | Treatment of inner ear hair cells |
| US5945126A (en) | 1997-02-13 | 1999-08-31 | Oakwood Laboratories L.L.C. | Continuous microsphere process |
| US5939421A (en) | 1997-07-01 | 1999-08-17 | Signal Pharmaceuticals, Inc. | Quinazoline analogs and related compounds and methods for treating inflammatory conditions |
| US6043221A (en) | 1997-07-30 | 2000-03-28 | Amgen Inc. | Method for preventing and treating hearing loss using a neuturin protein product |
| NZ504108A (en) | 1997-09-26 | 2002-06-28 | Noven Pharma | Bioadhesive compositions comprising a polyvinylpyrrolidone polymer and methods for topical administration of active agents |
| US6201072B1 (en) | 1997-10-03 | 2001-03-13 | Macromed, Inc. | Biodegradable low molecular weight triblock poly(lactide-co- glycolide) polyethylene glycol copolymers having reverse thermal gelation properties |
| US6004573A (en) | 1997-10-03 | 1999-12-21 | Macromed, Inc. | Biodegradable low molecular weight triblock poly(lactide-co-glycolide) polyethylene glycol copolymers having reverse thermal gelation properties |
| US6117949A (en) | 1998-10-01 | 2000-09-12 | Macromed, Inc. | Biodegradable low molecular weight triblock poly (lactide-co-glycolide) polyethylene glycol copolymers having reverse thermal gelation properties |
| US5985848A (en) | 1997-10-14 | 1999-11-16 | Albert Einstein College Of Medicine Of Yeshiva University | Inhibitors of nucleoside metabolism |
| IL135774A0 (en) | 1997-10-22 | 2001-05-20 | Ponikau Jens | Use of antinfungal agents for the topical treatment of fungus-induced mucositis |
| DE19748763A1 (en) | 1997-11-05 | 1999-05-06 | Hans Peter Zenner | Use of vasopressin antagonists |
| SE9704186D0 (en) * | 1997-11-14 | 1997-11-14 | Astra Ab | New composition of matter |
| US6177434B1 (en) * | 1997-12-16 | 2001-01-23 | The United States Of America As Represented By The Secretary Of The Navy | Prevention or reversal of sensorineural hearing loss (SNHL) through biologic mechanisms |
| US6649621B2 (en) * | 1997-12-16 | 2003-11-18 | The United States Of America As Represented By The Secretary Of The Navy | Prevention or reversal of sensorineural hearing loss (SNHL) through biologic mechanisms |
| GB9812426D0 (en) | 1998-06-10 | 1998-08-05 | Reckitt & Colmann Prod Ltd | Improvements in or relating to organic compositions |
| US6316011B1 (en) * | 1998-08-04 | 2001-11-13 | Madash, Llc | End modified thermal responsive hydrogels |
| US20020009478A1 (en) | 1998-08-24 | 2002-01-24 | Douglas Joseph Dobrozsi | Oral liquid mucoadhesive compositions |
| US6319513B1 (en) | 1998-08-24 | 2001-11-20 | The Procter & Gamble Company | Oral liquid mucoadhesive compounds |
| EP1107791B8 (en) | 1998-09-04 | 2007-11-07 | Scios Inc. | Hydrogel compositions for the controlled release administration of growth factors |
| US6740664B2 (en) * | 1998-09-30 | 2004-05-25 | Alcon, Inc. | Methods for treating otic and ophthalmic infections |
| US6270802B1 (en) | 1998-10-28 | 2001-08-07 | Oakwood Laboratories L.L.C. | Method and apparatus for formulating microspheres and microcapsules |
| US8197461B1 (en) * | 1998-12-04 | 2012-06-12 | Durect Corporation | Controlled release system for delivering therapeutic agents into the inner ear |
| US6451346B1 (en) * | 1998-12-23 | 2002-09-17 | Amgen Inc | Biodegradable pH/thermosensitive hydrogels for sustained delivery of biologically active agents |
| JP3572570B2 (en) | 1999-02-01 | 2004-10-06 | オーテックス株式会社 | Polymerization initiator for cationically polymerizable organic substances |
| ATE425165T1 (en) | 1999-04-08 | 2009-03-15 | Ind Res Ltd | METHOD FOR PREPARING NUCLEOSIDE METABOLISM INHIBITORS |
| US6287588B1 (en) | 1999-04-29 | 2001-09-11 | Macromed, Inc. | Agent delivering system comprised of microparticle and biodegradable gel with an improved releasing profile and methods of use thereof |
| JP2003501043A (en) | 1999-05-28 | 2003-01-14 | ターゲティッド ジェネティクス コーポレイション | Methods and compositions for reducing levels of tumor necrosis factor (TNF) in TNF-related disorders |
| MXPA01012283A (en) | 1999-06-23 | 2002-07-30 | Aventis Pharma Gmbh | Substituted benzimidazole. |
| US20040082509A1 (en) * | 1999-10-12 | 2004-04-29 | Christophe Bonny | Cell-permeable peptide inhibitors of the JNK signal transduction pathway |
| US6458387B1 (en) | 1999-10-18 | 2002-10-01 | Epic Therapeutics, Inc. | Sustained release microspheres |
| DE19951360A1 (en) | 1999-10-26 | 2001-05-03 | Aventis Pharma Gmbh | Substituted indoles |
| US7151191B2 (en) | 2000-01-13 | 2006-12-19 | Emisphere Technologies, Inc. | Compounds and compositions for delivering active agents |
| GB0003154D0 (en) | 2000-02-12 | 2000-04-05 | Astrazeneca Uk Ltd | Novel compounds |
| WO2001068648A1 (en) | 2000-03-15 | 2001-09-20 | Aventis Pharma Deutschland Gmbh | Substituted beta-carbolines with ikb-kinase inhibiting activity |
| WO2001072298A1 (en) * | 2000-03-27 | 2001-10-04 | The General Hospital Corporation | Treatments for immune-mediated ear disorders |
| US7758888B2 (en) | 2000-04-21 | 2010-07-20 | Sol-Gel Technologies Ltd. | Composition exhibiting enhanced formulation stability and delivery of topical active ingredients |
| US6589549B2 (en) | 2000-04-27 | 2003-07-08 | Macromed, Incorporated | Bioactive agent delivering system comprised of microparticles within a biodegradable to improve release profiles |
| US7018645B1 (en) | 2000-04-27 | 2006-03-28 | Macromed, Inc. | Mixtures of various triblock polyester polyethylene glycol copolymers having improved gel properties |
| US20020013331A1 (en) | 2000-06-26 | 2002-01-31 | Williams Robert O. | Methods and compositions for treating pain of the mucous membrane |
| US7289110B2 (en) * | 2000-07-17 | 2007-10-30 | Human Messaging Ab | Method and arrangement for identifying and processing commands in digital images, where the user marks the command, for example by encircling it |
| UA81743C2 (en) | 2000-08-07 | 2008-02-11 | Центокор, Инк. | HUMAN MONOCLONAL ANTIBODY WHICH SPECIFICALLY BINDS TUMOR NECROSIS FACTOR ALFA (TNFα), PHARMACEUTICAL MIXTURE CONTAINING THEREOF, AND METHOD FOR TREATING ARTHRITIS |
| AU2001284564A1 (en) | 2000-08-29 | 2002-03-13 | Albert Einstein College Of Medicine Of Yeshiva University | Nucleoside metabolism inhibitors |
| JP4272338B2 (en) | 2000-09-22 | 2009-06-03 | バイエル アクチェンゲゼルシャフト | Pyridine derivatives |
| IL145584A0 (en) * | 2000-10-02 | 2002-06-30 | Pfizer Prod Inc | Nmda nr2b antagonists for treatment |
| WO2002030353A2 (en) | 2000-10-12 | 2002-04-18 | Smithkline Beecham Corporation | NF-λB INHIBITORS |
| EP1328272A1 (en) | 2000-10-12 | 2003-07-23 | SmithKline Beecham Corporation | Nf-kappa-b inhibitors |
| EP1333834B1 (en) | 2000-10-26 | 2008-04-23 | Amgen Inc. | Antiinflammation agents |
| US20040018228A1 (en) * | 2000-11-06 | 2004-01-29 | Afmedica, Inc. | Compositions and methods for reducing scar tissue formation |
| JP2002193938A (en) | 2000-12-01 | 2002-07-10 | Bayer Ag | 4-arylpyridine derivative |
| US7122544B2 (en) | 2000-12-06 | 2006-10-17 | Signal Pharmaceuticals, Llc | Anilinopyrimidine derivatives as IKK inhibitors and compositions and methods related thereto |
| EP1370139A4 (en) | 2001-01-04 | 2010-09-22 | Einstein Coll Med | Inhibitors of adp-ribosyl transferases, cyclases, and hydrolases, and uses thereof |
| SE0100158D0 (en) | 2001-01-19 | 2001-01-19 | Synphora Ab | Novel method and composition for local treatment of Meniere's disease and tinnitus |
| WO2002060386A2 (en) | 2001-02-01 | 2002-08-08 | Bristol-Myers Squibb Company | METHODS OF TREATING INFLAMMATORY AND IMMUNE DISEASES USING INHIBITORS OF IλB KINASE (IKK) |
| US20060269602A1 (en) * | 2001-04-13 | 2006-11-30 | Dasch James R | Method of modifying the release profile of sustained release compositions |
| WO2002094265A1 (en) | 2001-05-24 | 2002-11-28 | Leo Pharma A/S | A method of modulating nf-$g(k)b activity |
| US20030045515A1 (en) | 2001-05-24 | 2003-03-06 | Lise Binderup | Combination medicament for treatment of neoplastic diseases |
| SE0102617D0 (en) | 2001-07-25 | 2001-07-25 | Astrazeneca Ab | Novel compounds |
| TWI324925B (en) | 2001-08-23 | 2010-05-21 | Novartis Ag | Ophthalmic composition |
| WO2003024936A1 (en) | 2001-09-19 | 2003-03-27 | Pharmacia Corporation | Substituted pyrazolo compounds for the treatment of inflammation |
| EP1444207A2 (en) | 2001-09-19 | 2004-08-11 | Pharmacia Corporation | Substituted pyrazolyl-compounds for the treatment of inflammation |
| WO2003029242A1 (en) | 2001-10-04 | 2003-04-10 | Smithkline Beecham Corporation | NF-λB INHIBITORS |
| AU2002356992A1 (en) | 2001-11-21 | 2003-06-10 | Albert Einstein College Of Medicine Of Yeshiva University | Sir2 products and activities |
| US7001615B1 (en) * | 2001-12-07 | 2006-02-21 | Alcon, Inc. | Sustained release ophthalmic, otic and nasal suspension |
| MXPA04005427A (en) | 2001-12-10 | 2005-04-19 | Amgen Inc | Vanilloid receptor ligands and their use in treatments. |
| TW200406390A (en) | 2002-01-17 | 2004-05-01 | Neurogen Corp | Substituted quinazolin-4-ylamine analogues |
| WO2003071986A2 (en) | 2002-02-22 | 2003-09-04 | Control Delivery Systems, Inc. | Method for treating otic disorders |
| JP2003277383A (en) | 2002-03-14 | 2003-10-02 | Bayer Ag | Optically active pyridine derivative and medicine containing the same |
| US7098334B2 (en) | 2002-03-25 | 2006-08-29 | Industrial Research Limited | 4-amino-5H-pyrrolo[3,2-d]pyrimidine inhibitors of nucleoside phosphorylases and nucleosidases |
| ES2355472T3 (en) | 2002-05-22 | 2011-03-28 | Amgen Inc. | AMINOPIRIMIDINE DERIVATIVES FOR USE AS VANILOID RECEIVER LINKS FOR PAIN TREATMENT. |
| US7022680B2 (en) | 2002-05-30 | 2006-04-04 | Albert Einstein College Of Medicine Of Yeshiva University | Inhibitors of ADP-ribosyl transferases, cyclases, and hydrolases |
| JP4555082B2 (en) | 2002-08-08 | 2010-09-29 | アムジエン・インコーポレーテツド | Vanilloid receptor ligands and their use in therapy |
| US7589110B2 (en) | 2002-09-06 | 2009-09-15 | Durect Corporation | Delivery of modulators of glutamate-mediated neurotransmission to the inner ear |
| US20060013858A1 (en) * | 2002-10-29 | 2006-01-19 | Trune Dennis R | Fludrocortisone treatment for hearing loss |
| US7220431B2 (en) * | 2002-11-27 | 2007-05-22 | Regents Of The University Of Minnesota | Methods and compositions for applying pharmacologic agents to the ear |
| US7582635B2 (en) | 2002-12-24 | 2009-09-01 | Purdue Pharma, L.P. | Therapeutic agents useful for treating pain |
| AU2003900887A0 (en) * | 2003-02-27 | 2003-03-13 | Novasel Australia Pty Ltd | Poloxamer emulsion preparations |
| US8802116B2 (en) * | 2003-02-27 | 2014-08-12 | Novasel Australia Pty. Ltd. | Poloxamer emulsion preparations |
| US20040185047A1 (en) | 2003-03-21 | 2004-09-23 | Jill Giles-Komar | Anti- TNF antibodies, compositions, methods and uses |
| EP1618102B1 (en) | 2003-04-21 | 2010-02-10 | Eli Lilly And Company | Substituted benzopyrans as selective estrogen receptor-beta agonists |
| ATE337003T1 (en) * | 2003-04-28 | 2006-09-15 | Biofrontera Bioscience Gmbh | USE OF RILUZOLE COMBINED WITH SUITABLE AGENTS AND ADDITIVES FOR THE TREATMENT OF DISEASES CHARACTERIZED BY HYPERPROLIFERATION OF KERATINOCYTES, IN PARTICULAR NEURODERMITIS AND PSORIASIS |
| US20040247575A1 (en) | 2003-06-03 | 2004-12-09 | Caplice Noel M. | Smooth muscle progenitor cells |
| US7329664B2 (en) | 2003-07-16 | 2008-02-12 | Neurogen Corporation | Substituted (7-pyridyl-4-phenylamino-quinazolin-2-yl)-methanol analogues |
| WO2005009987A1 (en) | 2003-07-24 | 2005-02-03 | Euro-Celtique S.A. | Piperidine compounds and pharmaceutical compositions containing them |
| MXPA06003615A (en) | 2003-09-30 | 2006-06-05 | Amgen Inc | Vanilloid receptor ligands and their use in treatments. |
| JP4947977B2 (en) * | 2003-10-31 | 2012-06-06 | わかもと製薬株式会社 | Reversible thermogelling aqueous composition |
| WO2005046438A2 (en) * | 2003-11-06 | 2005-05-26 | Pluromed, Inc. | Internal clamp for surgical procedures |
| US20050137122A1 (en) | 2003-12-17 | 2005-06-23 | Alcon, Inc. | Use of agents that prevent generation of amyloid and amyloid-like lipoproteins, and/or use of agents that promote sequestration and/or degradation of, and/or prevent neurotoxicity of such proteins in the treatment of hearing loss and improving body balance |
| US7312330B2 (en) | 2003-12-24 | 2007-12-25 | Renovis, Inc. | Bicycloheteroarylamine compounds as ion channel ligands and uses thereof |
| TW200530235A (en) | 2003-12-24 | 2005-09-16 | Renovis Inc | Bicycloheteroarylamine compounds as ion channel ligands and uses thereof |
| JP2005220070A (en) | 2004-02-05 | 2005-08-18 | Medgel Corp | Bioabsorbable polymer hydrogel preparation for neurotization and neuroprotection |
| US8268866B2 (en) | 2004-03-29 | 2012-09-18 | Matthieu Guitton | Methods for the treatment of tinnitus induced by cochlear excitotoxicity |
| US20060063802A1 (en) | 2004-03-29 | 2006-03-23 | Matthieu Guitton | Methods for the treatment of tinnitus induced by cochlear excitotoxicity |
| WO2005113544A1 (en) | 2004-05-12 | 2005-12-01 | Aventis Pharmaceuticals Inc. | Substantially pure 2-{[2-(2-methylamino-pyrimidin-4-yl)-1h-indole-5-carbonyl]-amino}-3-(phenylpyridin-2-yl-amino)-propionic acid as an ikb kinase inhibitor |
| CA2568028A1 (en) | 2004-05-24 | 2005-12-08 | Auris Medical, Llc. | Combined otic aspirator and medication dispenser |
| US20060034889A1 (en) | 2004-08-16 | 2006-02-16 | Macromed, Inc. | Biodegradable diblock copolymers having reverse thermal gelation properties and methods of use thereof |
| US20060046970A1 (en) * | 2004-08-31 | 2006-03-02 | Insite Vision Incorporated | Topical otic compositions and methods of topical treatment of prevention of otic infections |
| JP2008515867A (en) * | 2004-10-05 | 2008-05-15 | メルツ・ファルマ・ゲゼルシヤフト・ミト・ベシュレンクテル・ハフツング・ウント・コンパニー・コマンデイトゲゼルシヤフト・アウフ・アクティーン | Novel cyclic and acyclic propenones for treating CNS disease |
| US8498681B2 (en) | 2004-10-05 | 2013-07-30 | Tomophase Corporation | Cross-sectional mapping of spectral absorbance features |
| US20060105967A1 (en) | 2004-11-18 | 2006-05-18 | Advanced Gene Technology, Corp. | Flavone derivatives as TNFalpha inhibitors or antagonists |
| WO2006076318A1 (en) | 2005-01-12 | 2006-07-20 | Aventis Pharmaceuticals Inc. | Monopotassium salt of an ikb kinase inhibitor |
| JP2008527002A (en) | 2005-01-13 | 2008-07-24 | サートリス ファーマシューティカルズ, インコーポレイテッド | Novel composition for preventing and treating neurodegenerative disorders and blood coagulation disorders |
| JP2008526997A (en) | 2005-01-14 | 2008-07-24 | ニューロジェン・コーポレーション | Heteroaryl substituted quinolin-4-ylamine analogs |
| WO2006079055A2 (en) * | 2005-01-24 | 2006-07-27 | Neurosystec Corporation | Apparatus and method for delivering therapeutic and/or other agents to the inner ear and to other tissues |
| CN101232885A (en) | 2005-01-25 | 2008-07-30 | 神经能质公司 | Substituted pyridazinyl- and pyrimidinyl-quinolin-4-ylamine analogues |
| US20060221197A1 (en) | 2005-03-30 | 2006-10-05 | Jung Edward K | Image transformation estimator of an imaging device |
| US7576099B2 (en) | 2005-02-28 | 2009-08-18 | Renovis, Inc. | Amide derivatives as ion-channel ligands and pharmaceutical compositions and methods of using the same |
| US8476319B2 (en) | 2005-03-10 | 2013-07-02 | 3M Innovative Properties Company | Methods of treating ear infections |
| DE602006009231D1 (en) | 2005-03-10 | 2009-10-29 | Pfizer | SUBSTITUTED N-SULFONYLAMINOPHENYLETHYL-2-PHENOXYACETAMIDE COMPOUNDS |
| US7312233B2 (en) | 2005-03-14 | 2007-12-25 | Renovis, Inc. | Amide derivatives as ion-channel ligands and pharmaceutical compositions and methods of using the same |
| WO2006097817A1 (en) | 2005-03-17 | 2006-09-21 | Pfizer Japan Inc. | N- (n-sulfonylaminomethyl) cyclopropanecarboxamide derivatives useful for the treatment of pain |
| JP2008534530A (en) | 2005-03-29 | 2008-08-28 | エボニック レーム ゲゼルシャフト ミット ベシュレンクテル ハフツング | Multiparticulate drug form containing pellets with a substance having a modulating effect on active ingredient release |
| WO2006129164A1 (en) | 2005-05-31 | 2006-12-07 | Pfizer Japan Inc. | Substituted aryloxy-n-bicyclomethyl acetamide compounds as vr1 antagonists |
| US20070021352A1 (en) * | 2005-07-20 | 2007-01-25 | Cypress Bioscience, Inc. | Prevention and treatment of hearing disorders |
| WO2007031098A1 (en) | 2005-09-12 | 2007-03-22 | Xigen S.A. | Cell-permeable peptide inhibitors of the jnk signal transduction pathway |
| ZA200803367B (en) | 2005-09-26 | 2009-09-30 | Piedmont Pharmaceuticals Llc | Methods for treatment and prevention of otitis media using chemical penetration enhancers to facilitate transmembrane drug delivery into the middle ear |
| EA200800950A1 (en) | 2005-09-26 | 2008-08-29 | ПЬЕДМОН ФАРМАСЬЮТИКАЛЗ ЭлЭлСи | METHODS OF TREATMENT AND PREVENTION OF AVERAGE OTITIS WITH THE APPLICATION OF IRON-SURFACE-ACTIVE SUBSTANCES TO FACILITATE TRANSMEMBRANE INTRODUCTION OF MEDICINAL EARS |
| CU20080044A7 (en) | 2005-09-28 | 2011-04-26 | Pharmaceutical compositions for the treatment of disorders of the inner ear. | |
| AU2006303037A1 (en) | 2005-10-21 | 2007-04-26 | Merz Pharma Gmbh & Co Kgaa | Chromenones and their use as modulators of metabotropic glutamate receptors |
| US7785834B2 (en) | 2005-11-10 | 2010-08-31 | Ercole Biotech, Inc. | Soluble TNF receptors and their use in treatment of disease |
| US20070110788A1 (en) | 2005-11-14 | 2007-05-17 | Hissong James B | Injectable formulation capable of forming a drug-releasing device |
| US20070178051A1 (en) * | 2006-01-27 | 2007-08-02 | Elan Pharma International, Ltd. | Sterilized nanoparticulate glucocorticosteroid formulations |
| JP4273235B2 (en) * | 2006-06-01 | 2009-06-03 | 国立大学法人 新潟大学 | Aquaporin 4 inhibitor |
| TW200819458A (en) * | 2006-06-23 | 2008-05-01 | Merz Pharma Gmbh & Co Kgaa | Metabotropic glutamate receptor modulators |
| CL2007001829A1 (en) | 2006-06-23 | 2008-01-25 | Smithkline Beecham Corp | N- [4-Chloro-2-hydroxy-3- (piperazine-1-sulfonyl) phenyl] -n- (2-chloro-3-fluorophenyl) urea P-toluenesulfonate; preparation process; pharmaceutical composition; pharmaceutical combination; and use in the treatment of a disease mediated by chemokine il-8, such as asthma and epoc. |
| US8377898B2 (en) | 2006-10-12 | 2013-02-19 | Idera Pharmaceuticals, Inc. | Immune regulatory oligonucleotide (IRO) compounds to modulate toll-like receptor based immune response |
| US20080103118A1 (en) * | 2006-10-27 | 2008-05-01 | Iomedix Development International Srl | Composition for improving blood cholesterol levels |
| CA2669693C (en) | 2006-11-15 | 2018-06-12 | Massachusetts Eye & Ear Infirmary | Generation of inner ear cells |
| WO2008131439A1 (en) | 2007-04-23 | 2008-10-30 | House Ear Institute | Treatment and/or prevention of presbycusis by modulation of metabotropic glutamate receptor 7 |
| AU2009239429B2 (en) | 2008-04-21 | 2013-08-29 | Otonomy, Inc. | Auris formulations for treating otic diseases and conditions |
| JP5551685B2 (en) | 2008-05-14 | 2014-07-16 | オトノミ―,インク. | Controlled release corticosteroid compositions and methods of treating otic disorders |
| US8822410B2 (en) * | 2008-05-19 | 2014-09-02 | Children's Medical Center Corporation | Tympanic membrane permeating ear drops and uses thereof |
| US8648119B2 (en) | 2008-05-23 | 2014-02-11 | Otonomy, Inc. | Controlled release immunomodulator compositions and methods for the treatment of otic disorders |
| CN101288643B (en) * | 2008-06-17 | 2012-11-14 | 杨喜鸿 | Gel composition containing tacrolimu and its preparation method and medicinal application |
| US8846770B2 (en) | 2008-06-18 | 2014-09-30 | Otonomy, Inc. | Controlled release aural pressure modulator compositions and methods for the treatment of OTIC disorders |
| US8349353B2 (en) | 2008-06-27 | 2013-01-08 | Otonomy, Inc. | Controlled release cytotoxic agent compositions and methods for the treatment of otic disorders |
| WO2010011466A2 (en) | 2008-06-27 | 2010-01-28 | Otonomy, Inc. | Controlled-release cns modulating compositions and methods for the treatment of otic disorders |
| RU2493828C2 (en) | 2008-07-14 | 2013-09-27 | Отономи, Инк. | Apoptosis modulating compositions with controlled release and methods of treating ear diseases |
| EP2306975A4 (en) | 2008-07-21 | 2012-10-31 | Otonomy Inc | Controlled-release otic structure modulating and innate immune system modulating compositions and methods for the treatment of otic disorders |
| US8784870B2 (en) | 2008-07-21 | 2014-07-22 | Otonomy, Inc. | Controlled release compositions for modulating free-radical induced damage and methods of use thereof |
| US8399018B2 (en) | 2008-07-21 | 2013-03-19 | Otonomy, Inc. | Controlled release ion channel modulator compositions and methods for the treatment of otic disorders |
| US8318817B2 (en) | 2008-07-21 | 2012-11-27 | Otonomy, Inc. | Controlled release antimicrobial compositions and methods for the treatment of otic disorders |
| US8496957B2 (en) | 2008-07-21 | 2013-07-30 | Otonomy, Inc | Controlled release auris sensory cell modulator compositions and methods for the treatment of otic disorders |
| US20100016450A1 (en) | 2008-07-21 | 2010-01-21 | Otonomy, Inc. | Controlled release delivery devices for the treatment of otic disorders |
| JP2012506436A (en) | 2008-10-22 | 2012-03-15 | ハウス イアー インスティトゥート | Treatment and / or prevention of inner ear diseases by modulation of metabotropic glutamate receptors |
| JP5376987B2 (en) | 2009-02-18 | 2013-12-25 | キヤノン株式会社 | Reticle manufacturing method and surface shape measuring apparatus |
| JP6395687B2 (en) * | 2015-10-16 | 2018-09-26 | 株式会社カプコン | Video generation method, video generation program, and video generation apparatus |
-
2009
- 2009-04-21 AU AU2009239429A patent/AU2009239429B2/en not_active Ceased
- 2009-04-21 MX MX2010011545A patent/MX2010011545A/en active IP Right Grant
- 2009-04-21 KR KR1020197006299A patent/KR20190026056A/en active Search and Examination
- 2009-04-21 KR KR1020107026019A patent/KR101449785B1/en not_active IP Right Cessation
- 2009-04-21 RU RU2010147298/15A patent/RU2499592C2/en not_active IP Right Cessation
- 2009-04-21 US US12/427,663 patent/US9132087B2/en not_active Expired - Fee Related
- 2009-04-21 KR KR1020137020483A patent/KR20130097813A/en not_active IP Right Cessation
- 2009-04-21 WO PCT/US2009/041320 patent/WO2009132050A2/en active Application Filing
- 2009-04-21 EP EP09734483.2A patent/EP2278999A4/en active Pending
- 2009-04-21 JP JP2011505264A patent/JP2011518195A/en active Pending
- 2009-04-21 KR KR1020207009042A patent/KR102340754B1/en active IP Right Grant
- 2009-04-21 KR KR1020167005563A patent/KR20160029870A/en not_active Application Discontinuation
- 2009-04-21 CN CN200980114124.XA patent/CN102014957B/en not_active Expired - Fee Related
- 2009-04-21 CN CN201410609757.0A patent/CN104491864A/en active Pending
- 2009-04-21 CA CA2721927A patent/CA2721927C/en not_active Expired - Fee Related
- 2009-04-21 KR KR1020217026035A patent/KR20210107137A/en not_active Application Discontinuation
- 2009-04-21 BR BRPI0910850-5A patent/BRPI0910850B1/en active IP Right Grant
-
2010
- 2010-10-07 IL IL208549A patent/IL208549A/en active IP Right Grant
-
2013
- 2013-12-04 JP JP2013251480A patent/JP6147653B2/en not_active Expired - Fee Related
-
2015
- 2015-06-19 US US14/745,160 patent/US10272034B2/en not_active Expired - Fee Related
- 2015-10-08 HK HK15109820.0A patent/HK1209055A1/en unknown
- 2015-11-04 JP JP2015217021A patent/JP6296565B2/en not_active Expired - Fee Related
-
2016
- 2016-04-14 US US15/099,336 patent/US10751281B2/en active Active
- 2016-04-15 US US15/130,597 patent/US20160228357A1/en not_active Abandoned
-
2017
- 2017-04-06 JP JP2017076319A patent/JP6544535B2/en active Active
- 2017-04-18 IL IL251768A patent/IL251768B/en unknown
-
2019
- 2019-03-11 JP JP2019044231A patent/JP2019085423A/en active Pending
- 2019-04-19 US US16/389,213 patent/US11123285B2/en active Active
-
2020
- 2020-03-19 US US16/824,646 patent/US11123286B2/en active Active
- 2020-06-19 JP JP2020106530A patent/JP2020147610A/en active Pending
-
2021
- 2021-08-18 US US17/405,992 patent/US20220040096A1/en not_active Abandoned
- 2021-08-18 US US17/405,990 patent/US20220040095A1/en active Pending
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11369607B2 (en) | 2014-09-03 | 2022-06-28 | The Brigham And Women's Hospital, Inc. | Compositions, systems, and methods for generating inner ear hair cells for treatment of hearing loss |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US11123286B2 (en) | Auris formulations for treating otic diseases and conditions | |
| US20200397907A1 (en) | Triglyceride otic formulations and uses thereof | |
| US11918653B2 (en) | Triglyceride otic formulations and uses thereof | |
| AU2020230269B2 (en) | Auris formulations for treating otic diseases and conditions | |
| AU2013254940A1 (en) | Auris formulations for treating otic diseases and conditions |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| WWE | Wipo information: entry into national phase |
Ref document number: 200980114124.X Country of ref document: CN |
|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 09734483 Country of ref document: EP Kind code of ref document: A2 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2009734483 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2721927 Country of ref document: CA Ref document number: 2011505264 Country of ref document: JP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: MX/A/2010/011545 Country of ref document: MX |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2009239429 Country of ref document: AU |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 8019/DELNP/2010 Country of ref document: IN |
|
| ENP | Entry into the national phase |
Ref document number: 20107026019 Country of ref document: KR Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2010147298 Country of ref document: RU |
|
| ENP | Entry into the national phase |
Ref document number: 2009239429 Country of ref document: AU Date of ref document: 20090421 Kind code of ref document: A |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01E Ref document number: PI0910850 Country of ref document: BR Free format text: APRESENTE DOCUMENTO DE CESSAO PARA TODAS AS PRIORIDADES REIVINDICADAS, UMA VEZ QUE O DOCUMENTO DE CESSAO APRESENTADO NA PETICAO NO 860150278094 E REFERENTE A SOMENTE AO PEDIDO US 12/427,663 E O DIREITO DE PRIORIDADE NAO PODE SER EXTRAPOLADO DE UM PEDIDO PARA OUTRO. A CESSAO DEVE CONTER, NO MINIMO, NUMERO DA PRIORIDADE A SER CEDIDA, DATA DE DEPOSITO DA PRIORIDADE E ASSINATURA DE TODOS OS INVENTORES. |
|
| ENP | Entry into the national phase |
Ref document number: PI0910850 Country of ref document: BR Kind code of ref document: A2 Effective date: 20101020 |